

REPORT OF THE
TASK FORCE ON FOOD ALLERGY AWARENESS, FOOD SAFETY, AND
FOOD SERVICE FACILITY LETTER GRADING
TO THE
MARYLAND GENERAL ASSEMBLY
IN FULFILLMENT OF CHAPTER 252
January 2014

Page 2
EXECUTIVE SUMMARY
The Task Force on Food Allergy Awareness, Food Safety, and Food Service Facility Letter
Grading (the Task Force) was established by the Department of Health and Mental Hygiene
(the Department) in 2013 to examine issues related to food service facilities in Maryland.
The Task Force developed a series of findings and recommendations that are detailed in this
report.
Food Safety: In the area of food safety related to safety training and manager
certification, the Task Force recommends that Maryland should move progressively
towards a requirement that a certified food protection manager must be present at all
facilities when food preparation and service to the general public is taking place.
Food Allergy Awareness: With respect to food allergies, the Task Force
recommends that by 6 months after implementation, food service facilities display on
their menus, menu boards or at the point of service the request that Patrons with
known food allergies notify their server of the allergies, prior to ordering food. The
Task Force also recommends that food service facilities have available at all times, on
their premises, a member of the staff, who has taken a food allergen awareness
training course, approved by the Department, and passed an accredited test, for
consultation with patrons to discuss meal options so as to minimize potential allergen
risks. The timing for this requirement is to be established by the Department in
regulation. The Department will post a list of acceptable third-party online and in-
person food allergen awareness training courses, and list resources for restaurants to
learn more about food safety and food handling as they relate to food allergies. The
Department will also initiate tracking of food allergy complaints as new resources are
made available to the Department to do so.
Food Service Facility Letter Grading: Finally, regarding letter grading of food
service facilities, the Task Force did not recommend adoption of any form of letter
grading or scoring of inspection reports of food service facilities. Rather, the Task
Force considered alternatives to letter grading, and encourages the routine publication
of those parts of facility inspection reports, which relate to those items, generally
known as the critical items, most closely related to public health. While the Task
Force did not specify a preference for a publication method, it did recognize that
resources would be required to support this activity.

Page 3
Contents
EXECUTIVE SUMMARY ...................................................................................................................................................................... 2
THE TASK FORCE CHARGE ................................................................................................................................................................ 4
MARYLAND FOOD SERVICE FACILITY OVERVIEW ..................................................................................................................... 5
Most Common Violations ................................................................................................................................................................... 6
Closure Actions ................................................................................................................................................................................... 6
Foodborne Illness Outbreaks in Maryland ........................................................................................................................................... 6
FOOD SAFETY TRAINING ................................................................................................................................................................... 8
Current Training .................................................................................................................................................................................. 8
Food Manager Certification National Training Courses and Examinations ........................................................................................ 8
Other States’ Activities ........................................................................................................................................................................ 9
Finding 1: Food Protection Manager Certification ............................................................................................................................. 9
Recommendation 1: Food Protection Manager Certification.............................................................................................................. 9
ALLERGEN AWARENESS .................................................................................................................................................................. 11
Clinical Syndromes and Public Health Impact .................................................................................................................................. 11
Food Service Facility Operational Issues .......................................................................................................................................... 11
State and Federal Legislation............................................................................................................................................................. 12
Massachusetts Allergen Law ............................................................................................................................................................. 13
The Americans with Disabilities Act Compliance, Legal Liability ................................................................................................... 14
Food Allergen Training in Maryland ................................................................................................................................................. 15
National Training Courses ................................................................................................................................................................. 15
Food Allergy Training Activities in Other States .............................................................................................................................. 15
Finding 2: Food Allergy Training ..................................................................................................................................................... 15
Recommendation 2: Food Service Facility Training and Prevention Recommendations Related to Food Allergies ....................... 15
GRADING AND CLASSIFYING HEALTH INSPECTION RESULTS ............................................................................................... 17
Current Maryland Practice ................................................................................................................................................................. 17
Other States’ Grading Practices ......................................................................................................................................................... 17
Alternative Public Outreach Methodologies ...................................................................................................................................... 18
Finding 3: Letter Grading of Food Service Facilities ....................................................................................................................... 19
Recommendation 3: Letter Grading of Food Service Facilities ......................................................................................................... 19
Recommendation 4: Alternatives to Letter Grading of Food Service Facilities ............................................................................... 19
APPENDIX 1: Task Force Membership ................................................................................................................................................. 20
APPENDIX 2: Chapter 252 – House Bill 9 (2013 Legislative Session) ................................................................................................. 21
APPENDIX 3: Task Force Activity Meetings ........................................................................................................................................ 25
APPENDIX 4: Overview of Issues Associated with Living with Food Allergies................................................................................... 26
APPENDIX 5: Massachusetts Allergen Law .......................................................................................................................................... 29
APPENDIX 6: AG’s Letter on Allergen Legal Summary ...................................................................................................................... 31
APPENDIX 7: Maryland Food Service Facility Inspection Form ......................................................................................................... 35
APPENDIX 8: New York City Food Service Facility Scoring Form ..................................................................................................... 37
APPENDIX 9: Los Angeles County Inspection and Scoring Form ........................................................................................................ 42
Page 4
THE TASK FORCE CHARGE
House Bill 9 (Chapter 252) was passed by the Maryland General Assembly in 2013. This legislation
created a Task Force (membership listed in Appendix 1) to study food allergy awareness, food
safety, and food service facility (FSF) letter grading (see full legislation in Appendix 2). The Task
Force was established to:
1. Study and make recommendations regarding:
● Food allergy awareness and food allergy training for food service facilities in the
State;
● Food safety training for food service facilities in the State; and
● The use of systems for grading and classifying health inspection results for food
service facilities in the State.
2. Review food safety efforts at the State and local level, including:
● The frequency of food service facility inspections, the most common violations, and
the reasons for closures;
● The number of foodborne illness cases that have been linked to food service facilities;
and
● The impact of local food service manager certification programs.
3. Study:
● The most common food allergies and issues related to food preparation and cross–
contamination in food service facilities;
● Existing and planned food allergy training materials, programs, and certifications;
● Food allergy awareness and training mandates for food service facilities in other
states;
● Legal issues related to food allergens, including potential civil liability, compliance
with the Americans with Disabilities Act, and negligence issues;
● The use of grading and classifying health inspection results for food service facilities
by other jurisdictions;
● The frequency of foodborne illness cases linked to food service facilities in
jurisdictions that grade and classify health inspection results compared to similar
jurisdictions that do not use grading and classification systems;
● The costs of implementing and administering grading and classifying systems, how
the costs of these systems are paid for, and any cost–benefit analyses of these systems
that have been completed;
● The alternatives to grading and classifying health inspection results, including the
State’s existing pass–fail inspection system, online posting of health inspection
results, a system that informs consumers regarding the frequency of health
inspections at food service facilities, and any other options the Task Force considers
appropriate.
4. Study and evaluate:
● Mandated food service manager certification and mandated food handler training
options; and

Page 5
● Online food safety training programs for certification and recertification.
The Task Force was directed to report its findings and recommendations on or before January 1,
2014. Because of the scope of the Task Force’s activities, this report presents its recommendations
with a significant portion of the supporting materials in the appendices.
MARYLAND FOOD SERVICE FACILITY OVERVIEW
The Department delegates to the 24 local health departments in the State the authority to inspect and
enforce approximately 27,000 food service facilities in accordance with the Code of Maryland
Regulations (COMAR) 10.15.03 – Food Service Facilities. These regulations mandate food service
facilities be inspected at a prescribed frequency associated with the risk of food handling involved
using a Hazard Analysis Critical Control Point (HACCP) approach to food safety. The inspections
ensure that the food service facilities are conducting business by ensuring certain critical items are
met. These items include:
Critical Items
Obtaining food from an approved source;
Protecting raw and ready-to-eat food from all adulteration, spoilage and contamination;
Restricting food workers with infection or other indicators of illness;
Ensuring that all food workers wash hands thoroughly before contact with utensils, raw food
and before using gloves;
Properly cooling and refrigerating potentially hazardous foods and providing sufficient
refrigeration equipment;
Holding potentially hazardous foods at proper hot temperatures and providing sufficient hot-
holding equipment;
Adequately cooking and reheating potentially hazardous foods;
Providing potable hot and cold running water; and
Discharging sewage properly from the facility.
A priority assessment is conducted for each food establishment based on the information provided at
the time of plan reviews, construction, remodeling, or any planned changes. Priority is established
by the complexity of food processes conducted at the establishment using the HACCP approach.
Types of Priority and Frequency of Inspections
● High priority food service facility: At a minimum frequency of three times per year,
one at every 4-month interval;
● Moderate priority food service facility: At a minimum of two times per year, one
every 6 months;
● Low priority food service facility: Using a comprehensive inspection at a minimum
of once every 2 years.

Page 6
The mandated inspections rate for each local health department is based on the number of food
service facilities in each priority area. Typically, with an adequately staffed program, completing
80% of the mandated inspections rate is a realistic achievement. In practice, the number of
Environmental Health Specialists (EHS) available in a jurisdiction to conduct routine food service
facility inspections is limited and reduced by unscheduled events such as complaints, foodborne
illness outbreaks, re-inspections to confirm corrective actions have been completed and requirements
to conduct mandated inspections/investigations in other Environmental Health programs.
Most Common Violations
A review of the most recent local health department inspection reports showed that the most
common critical violations were:
● Failure to hold hot foods above 135 degrees F to minimize microbial growth; and
● Failure to hold cold foods below 41 degrees F to minimize microbial growth.
Closure Actions
A recent sampling of several local health department records showed the following number of
facility closures during the last fiscal year:
● Baltimore City - 109 facilities
● Baltimore County - 32 facilities
● Caroline County - 3 facilities
● Cecil County - 3 facilities
● Howard County - 20 facilities
● Kent County - 3 facilities
● Montgomery County -30 facilities
● Prince Georges County – 80 facilities
● Wicomico County - 5 facilities.
It should be noted that the number of facilities in each jurisdiction varies depending on location and
population. The above figures do not reflect the number of critical item violations in a jurisdiction.
If a critical item violation is corrected immediately during the inspection then the facility is not
closed. Also, not all of the closures reflect food related issues, but may be caused by events external
to the facility such as broken water mains and floods.
Foodborne Illness Outbreaks in Maryland
In accordance with COMAR, all illness outbreaks are reported to the Office of the State
Epidemiologist within the Department. For foodborne illnesses, a foodborne outbreak in Maryland
is defined as:
● Two or more epidemiologically linked cases of illness following the consumption of a
common food item or items; or
● One case of botulism, cholera, mushroom poisoning, trichinosis or fish poisoning.

Page 7
State epidemiologists also monitor a number of
national databases sponsored by the U.S. Food and
Drug Administration (FDA) and the Centers for
Disease Control and Prevention (CDC), such as
PulseNet and FoodNet, to facilitate interstate
coordination of outbreaks that cross state lines.
Figure 1 shows the number of foodborne outbreaks
reported to the Department from 2000-2012 and
shows a significant reduction of foodborne outbreaks
over this time period.
Figure 2 provides a breakdown of foodborne
outbreaks by attributed source and shows that
restaurants are the largest single source of
outbreaks. However, while food service facilities
are the major attributed source of foodborne
outbreaks they may often not be the primary cause
of the outbreak. Frequently food service facilities
become the focus of a foodborne outbreak, not
because of failures in their operating practices, but
because the food they served was already
contaminated when they received it and they
provided it to a sufficient number of customers
who became ill. Over the last decade national
foodborne outbreaks have become a significant
feature of the food industry due to the integration
and efficiency of the food supply industry.
Figure 3 shows a breakdown of the foodborne outbreaks by the organism responsible. From 2003-
2012 only 26% of the foodborne outbreaks had their organism source determined although in more
recent years this has increased close to 100%
in keeping with CDC and FDA
guidelines.Dramatic improvements have
been made in establishing organism
serotypes by “DNA fingerprinting”
techniques.
Figure 1. Foodborne outbreaks reported to Maryland
Department of Health and Mental Hygiene, 2000-2012
Figure 3. Foodborne Illness Outbreaks by Etiology, 2003-2012
Figure 2. Foodborne Illness Outbreaks by exposure site, 2003-
2012

Page 8
FOOD SAFETY TRAINING
Current Training
The Department conducts standardization of at least one EHS in each of the 24 jurisdictions.
Standardization is a process of training and evaluation designed to promote uniformity among retail
food inspection staff in the interpretation of laws and regulations during food facility inspections.
The goal is to provide consistency throughout the State with inspections and enforcement
procedures. The local standardization officer (LSO) is then required to train their staff on the same
HACCP inspection protocols. In general, the State and local health departments do not provide
regular training courses onfood safety but will, in the event of a food safety issue, work with
individual facilities on re-training staff as a method of overcoming persistent operational
weaknesses. The exception to this is when significant changes occur in the State law and food safety
regulations. In those circumstances, outreach programs are initiated to make the food industry aware
of the changing regulations.
Currently, five local health departments in Maryland have established Food Manager Certification
programs; Baltimore City, Montgomery, Prince Georges, Howard and Baltimore Counties. These
municipalities formed the Inter-jurisdictional Certified Food Manager Committee (the Committee),
which meets to discuss and establish operational procedures in accordance with their local statutes.
The Committee also maintains a database of course instructors who can provide food safety training
to food service facilities, for a negotiable fee, in a variety of languages. Prince Georges and
Baltimore Counties also have a limited certified food manager training course available for non-
profit organizations that meet certain criteria at a minimal fee or no charge respectively.
Food Manager Certification National Training Courses and Examinations
There are many courses available to teach individuals in the food service industry about food safety
and prepare them for a Conference of Food Protection accredited examination (ANSI/CFP) to
become a Certified Food Protection Manager. The National Restaurant Association (NRA), Food
Marketing Institute, National Environmental Health Association and others provide third party
training courses for food service facility employees that rely on the most current FDA Food Code as
well the CDC’s foodborne illness reports. There are currently four ANSI/CFP examination providers
in the nation:
Learn2Serve;
National Registry of Food Safety Professionals;
National Restaurant Association/ ServSafe; and
Prometric, Inc.
Each provider follows the same standards to ensure consistency in the way the examination is
created and the topics covered as well as how they are administered to individuals.

Page 9
Other States’ Activities
A web-based survey of a number of states across the country indicates that most states do not
operate regular general training courses but work with individual facilities on training when
necessary to resolve persistent issues.
The biggest training trend across many states is to adopt a formal certification requirement for food
service facilities in the form of Food Protection Manager Certification. The following studies by the
FDA provide more information on this issue:
http://www.fda.gov/Food/GuidanceRegulation/RetailFoodProtection/FoodborneIllnessRi
skFactorReduction/ucm224334.htm ; and
http://www.fda.gov/Food/GuidanceRegulation/RetailFoodProtection/FoodborneIllnessRi
skFactorReduction/ucm093797.htm#new
These studies have shown that adopting Food Protection Manager certification requirements can
significantly reduce the incidence of foodborne illness outbreaks at food service facilities. The
details were established by the Conference for Food Protection and can be found in the current
version of the Food Code as follows:
“2-102.12 Certified Food Protection Manager
(A) At least one employee that has supervisory and management responsibility and the
authority to direct and control food preparation and service shall be a certified food
protection manager who has shown proficiency of required information through passing a
test that is part of an accredited program.”
The certification program is one that has been evaluated and listed by a Conference for Food
Protection-recognized accrediting agency as conforming to the Conference for Food Protection
Standards for Accreditation of Food Protection Manager Certification.
Finding 1: Food Protection Manager Certification
Based on evidence provided to the Task Force, Maryland has significantly reduced the incidence of
foodborne illness outbreaks in the past decade, but the downward trend has leveled off in recent
years. The FDA has found that adopting Food Protection Manager Certification provides a vehicle
that could further reduce the incidence of foodborne illness outbreaks at food service facilities.
Recommendation 1: Food Protection Manager Certification
Based on the findings above, the Task Force recommends:
1. A food service facility must have on the premises at all times an ANSI-CFP Certified Food
Protection Manager.
The Task Force recommends that the food service facilities in Maryland progressively move to a
position where a certified food protection manager must be present at all facilities when food

Page 10
preparation and service to the general public is taking place. The Department will establish, in
regulation, the transition time and requirements for compliance with this regulation. The
Department will post on its website a list of third-party training courses which can be taken to
prepare for the required certification examination.
The Task Force also encourages local health departments, at their own discretion, to explore low
cost options to assist non-profit organizations in obtaining the necessary training and certification to
comply with the Certified Food Protection Manager regulation.

Page 11
ALLERGEN AWARENESS
Clinical Syndromes and Public Health Impact
The prevalence of food allergies in America is estimated to be around 8% in children
1
somewhere
less than 10% in the populations as a whole.
2
The number of people with food allergies appears to
be growing, but explanations for the increase are uncertain, and studies are complicated by
inconsistent case definitions. According to a study released in 2013 by the CDC, food allergies
among children 0 – 17 years of age increased from 3.4% to 5.1%, an increase of 50%, between 1997
and 2011.
3
The eight most common food allergens, which account for 90% of food allergies,
include cow’s milk, eggs, peanuts, tree nuts, fish, shellfish, soy and wheat.
4
When an individual
with a food allergy consumes food containing their allergen, the spectrum of reactions may range
from mild to severe. Symptoms may range from itching and tingling all the way to severe and
potentially fatal reactions such as anaphylaxis involving circulatory collapse and cardiac arrest.
Although scientific studies are ongoing, there is currently no preventive treatment or cure for food
allergies; only strict avoidance will avert a reaction. Although specific estimates are unavailable for
Maryland, a recent study estimated the national cost of food allergies in 2007 was $225 million in
direct medical services, with another $115 million in indirect costs.
5
See Appendix 4 for a more detailed overview of the issues associated with living with allergies.
Food Service Facility Operational Issues
Most food service facilities are designed to provide a hygienic environment in which food can be
safely prepared, cooked and served to customers. As such the primary focus of a food service
facility is to minimize the risk of microbial contamination of prepared food. This is achieved by
adequate sanitation of the facilities, cooking to the appropriate temperatures and avoiding cross-
contamination between raw and ready to eat products during service and preparation.
Allergens require a new awareness by food service facilities that can necessitate a more
individualized approach to minimize the risk of potentially hazardous cross-contact. This approach
will require knowledge of the ingredients of all food components in the facility and strategies to
minimize cross-contact risks at all stages, in food storage, preparation and serving for food allergic
individuals.
1
Gupta RS, Springston EE, Warrier MR, Smith B, Kumar R, Pongracic J, Holl JL. The prevalence, severity, and
distribution of childhood food allergy in the United States. Pediatrics. 2011 Jul;128(1):e9-17. doi: 10.1542/peds.2011-
0204. Epub 2011 Jun 20.
2
Chafen JJ, Newberry SJ, Riedl MA, Bravata DM, Maglione M, Suttorp MJ, Sundaram V, Paige NM, Towfigh A,
Hulley BJ, Shekelle PG. Diagnosing and managing common food allergies: a systematic review. JAMA. 2010 May
12;303(18):1848-56. doi: 10.1001/jama.2010.582.
3
U.S. National Center for Health Statistics. Trends in Allergic Conditions Among Children: United States, 1997–2011.
NCHS Data Brief (No. 121), May 2013. Accessed 12/22/2013 at: http://www.cdc.gov/nchs/data/databriefs/db121.pdf.
4
3.Boyce JA, Assa'ad A, Burks AW, et al; NIAID-Sponsored Expert Panel. Guidelines for the diagnosis and
management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol.
2010;126(suppl 6):S1-S58.
5
Patel DA, Holdford DA, Edwards E, et al.. Estimating the economic burden of food-induced allergic reactions and
anaphylaxis in the United States. J Allergy Clin Immunol. 2011; 128: 110–115.

Page 12
Some food service facilities will be unable to provide an accommodation for certain food-allergic
patrons, because their featured concept or product may include a food allergen as the main ingredient
of what they promote as a popular food product.
Federal Guidance: The Food Code
Reference to the current version of the Food Code (2013) provides some guidance on food allergies.
Section 2-103.11 (M) of the Food Code requires that employees are properly trained in food safety,
including food allergy awareness, as it relates to their assigned duties. It is important to note that the
Food Code only focuses on the eight major food allergens and does not address food allergens in
general. The Annex to the Food Code amplifies this, indicating that restaurant and retail food
service managers need to be aware of the serious nature of food allergies, including allergic
reactions, anaphylaxis, and death. It also indicates that restaurant and retail food service managers
need to:
● Know the eight major food allergens (listed above), which account for 90% of
allergies;
● Understand food allergen ingredient identities and labeling; and
● Avoid cross-contact during food preparation and service.
The Annex also indicates that allergens fall under the category of potential chemical hazards.
It is important to remember, however, that the Food Code is not a regulation or federal law, but
simply a Model Ordinance designed and provided for individual states use as a basis for state laws
and regulations.
State and Federal Legislation
Currently, Maryland’s only state law relating to food allergy awareness is Chapter 262, HB9 (2013).
This statute created the Task Force and the requirement to post allergen awareness posters.
At the federal level, two statutes exist which relate to allergens in food:
● Food Allergen Labeling and Consumer Protection Act of 2004 (FALCPA);
● FDA Food Safety Modernization Act of 2011 (FSMA)
FALCPA only applies to packaged food items and as such does not apply to food service facilities.
It is, however, instructive for the insight it gives into legislative thinking on allergens:
● The Legislation only applies to the designated eight foods known collectively as the
“major food allergens”. The FDA notes this group of allergens accounts for 90% of
all food allergies. Although there are other foods to which sensitive individuals may
react, the labels of packaged foods containing these other allergens are not required to
be in compliance with FALCPA”.
● FALCPA did not require the FDA to establish a threshold level for any food allergen.

Page 13
FSMA amends Chapter IV (21 U.S.C. 341 et seq.) such that the operator of a facility should have a
written plan that:
● Identifies and evaluates known and reasonably foreseeable hazards associated with
the facility;
● Identifies and implements preventive controls to minimize the risks;
● Monitors the effectiveness of the controls;
● Establishes corrective actions for failures of the preventative controls;
● Verifies the functioning of the plan; and
● Maintains records to demonstrate the correct functioning of the risk management
plan.
Allergens are included in the list of foreseeable hazards to be evaluated in the risk management plan.
At the state level, the State of Massachusetts has enacted an Allergy Awareness Bill. This law
requires food service facilities to:
Display an educational poster in the employee work area covering allergens and related
issues;
Display on menus, menu boards or at the point of service the following “Before placing
your order, please inform your server if a person in your party has a food allergy”; and
Have at least one certified food protection manager to have a food allergen awareness
training certificate.
The State of Rhode Island has recently passed similar legislation. Additionally, Illinois, Connecticut,
and New York have legislation that is currently being considered and pending legislative action as
follows:
● Illinois Senate Bill 37 which would mirror the MA Food Allergy Awareness Act;
● Connecticut Senate Bill 263 which would mirror the MA Food Allergy Awareness
Act;
● Connecticut Senate Bill 895 which would require restaurants to establish written
procedures to serve customers with food allergies; and
● New York Senate Bill 214 which would:
○ Require the creation of a food allergy poster by the department of health;
○ Require the posting of the food allergy poster in all food service
establishments; and
○ Authorize the department to charge a fee to cover printing, postage and
handling expenses of the posters.
Massachusetts Allergen Law
The full details of the Allergen Awareness Act, M.G.L. c. 140, § 6B, can be found in. Appendix 5
together with a link to the frequently asked questions and other guidance released by the
Massachusetts Department of Public Health (MDPH) Public Health Council.

Page 14
The Americans with Disabilities Act Compliance, Legal Liability
Disclaimer: The following section of the report is a brief summary of the potential
significance of legal topics related to allergens but is not a legal opinion on any of the items
covered.
In the absence of specific legislation, consumers with food allergies have used a variety of
approaches to seek redress for an allergen reaction including:
● Common law product liability actions;
● Failure to warn of a product or manufacturing defect;
● State consumer protection laws; or
● The Americans with Disabilities Act (ADA).
These actions appear to have met with little success, although recent amendments to the ADA may
have some impact in the allergen area and food allergies have now been interpreted to be a disability
under the law. However, overall there is little history of food allergen litigation in the United States
of America.
In response to an inquiry from the Task Force, the Office of the Attorney General indicated
(Appendix 6) that it is likely that the Task Force proposals do not create any new legal cause of
action for restaurant consumers or expose restaurants owners to new legal liability.
Food Allergen Training
While a significant number of restaurants operate on a “cook-to-order” basis, which often gives them
the flexibility to accommodate food-allergic customers, restaurant employees generally receive little
or no training on the serious nature of food allergies. As a result, restaurant staff often cannot
accurately respond to inquiries from food-allergic customers or help them select safe menu items and
may be vastly misinformed.
In a survey given to one hundred restaurant personnel, including managers, chefs, and wait-staff,
one-quarter of the respondents incorrectly indicated that removing an allergen from a finished meal
(e.g., taking off nuts) was safe; and one-quarter incorrectly indicated that consuming a small amount
of an allergen would be safe. This lack of understanding could have life threatening consequences
for customers with food allergies.
6
Restaurants recognize the importance of education in this area. According to a survey by the
National Restaurant Association, some 87% of restaurants believe food allergies are extremely
important and expect increased attention to it. Yet 43% concede they do not train their staff on food
allergens.
7
6
Source: Pre-publication information presented by National Restaurant Association Task Force member.
7
Source: Pre-publication information presented by National Restaurant Association Task Force member.

Page 15
Food Allergen Training in Maryland
Currently, there is no requirement in the State of Maryland for retail food service facilities to have
training on food allergen awareness. Additionally, there is no statewide training that covers food
allergen awareness for food service facilities.
National Training Courses
While there are a number of food allergen related training courses available from third parties there
are very few food allergen awareness courses that focus on food service operations. The first of
these has been established by the National Restaurant Association and it is anticipated that additional
courses will become available as more states address food allergen issues.
Food Allergy Training Activities in Other States
A survey of states with pending food allergen related legislation indicated that these states are
looking at training activities used in Massachusetts as a model for their training programs, as there
are not many other programs available at this time. A concern many states have is that there are few
options available for people who speak English as a second language and these states are looking at
the training industry to create programs, either online or in classrooms that can accommodate this
need.
Finding 2: Food Allergy Training
Allergen mediated health issues impact a growing segment of the population of the United States
and Maryland. At present, there is no Maryland law or regulation that places allergen awareness
training requirements on food service facilities.
The Department does not currently track reports of food allergy reactions but does include food
allergy questions in its foodborne illness investigations.
Recommendation 2: Food Service Facility Training and Prevention Recommendations Related to
Food Allergies
The following recommendations are made to promote education and awareness of food allergies in
food service facilities. They are not intended to require restaurants to alter their recipes to
accommodate food allergic customers, only to educate staff about food allergies so they may better
respond to consumers’ inquiries. This may mean in some cases, after consulting with a food allergic
individual, the restaurant in conjunction with the patron may determine that the restaurant is not able
to safely meet the needs of the patron.
The Task Force recommends that:

Page 16
1. By six months after implementation, food service facilities display on their menus, menu
boards or at the point of service the request that patrons with known food allergies notify
their server of the allergies, prior to ordering food;
2. Food service facilities have available at all times, on their premises, a member of the
staff, who has taken a food allergen awareness training course, approved by the
Department, and passed an accredited test, for consultation with patrons to discuss meal
options so as to minimize potential allergen risks. The timing for this requirement is to
be established by the Department in regulation;
3. The Department will provide and post on its website a list of acceptable third-party online
and in-person food allergen awareness training courses consistent with ANSI-ASTM
2659. Additionally, the Department will also list resources for restaurants and consumers
to learn more about food safety and food handling protocol as it relates to food allergies;
and
4. The Department will initiate tracking of food allergy reactions as new resources are made
available for the Department to do so.

Page 17
GRADING AND CLASSIFYING HEALTH INSPECTION RESULTS
Current Maryland Practice
Food service facilities in Maryland are regulated under COMAR 10.15.03, Food Service Facilities.
Facility inspections are based on the HACCP methodology and an inspection form that is in general
use by the local health department (see Appendix 7). The inspection form has two main components
with the first section covering those items that are most closely linked to public health and
collectively known as the critical items. The second segment is comprised of Good Retail Practice
(GRP) items that contribute to general safe operation of the facility. Each item that is observed
during the inspection is designated as a “pass” or a “fail” depending on whether the items complies
with regulatory requirements or not. For items in the critical section of the form, in the event of a
“fail” the item must be corrected immediately or the facility is closed. For items in the GRP section
of the form a correction plan is developed by the facility staff and a completion time for the
corrective action is given by the EHS. A follow-up inspection may be used to verify the GRP items
have been corrected as agreed or by the next routine inspection.
Other States’ Grading Practices
A number of jurisdictions across the country have introduced letter grading of inspections as a
means of public outreach. New York City and Los Angeles County in California represent the two
most widely known systems currently in use. (Appendix 8 and 9). A detailed review of these two
typical letter grading schemes shows that:
● In general not all of the items on the inspection report are scored, which can lead to
de-emphasis of the non-scored items and influence facility safety;
● Depending on the methodology, some items of the inspection occur more than once in
the scoring system leading to choice in how the item is scored or allowing for double
scoring under some circumstances;
● There is no general agreement on what numerical value or “weight” is assigned to
specific items on the inspection report; and
● There is no general agreement on how the actual scores are assigned a given letter
grade so differences may occur between jurisdictions or states.
Overall, there is no clear indication of how a grade A facility differs from a grade B facility or how
this relates to the average jurisdiction inspection grade. It is also not clear how the grade impacts
public health risks for patrons. The grade could be the result of a larger number of more lower
scored items, for example related to GRP issues or a very small number of highly scored critical
items. There is a large risk that the general public with its general familiarity with Grade A, Grade
B, etc., ratings may be misled into reading more into the grade than is warranted.
At this time, there is no significant independent body of information that could support the idea that
the introduction of letter grading has led to a significant reduction in foodborne illness outbreaks
associated with food service facilities.

Page 18
While no definitive costs have been published, it does appear that adding the additional step of letter
grading, inspection reports will require more resources on behalf of the inspecting agency and may
lead to more frequent requests for re-inspections as food service facilities strive to improve a
grading.
Among the concerns expressed on behalf of the Environmental Health Specialists, who inspect food
service facilities were:
Assigning a “grade” to an inspection report could lead to the creation of false
expectations with the public at large;
The grade could quickly become a “marketing” tool;
Pressure to get a “good grade” could shift the focus of inspections away from the current
focus on public health;
Limited inspection resources could be overloaded by facilities requesting frequent re-
inspections to improve their grading; and
Facility/Inspector relationships could be degraded by pressures to achieve a desired score,
particularly if the scoring system has a range of scores that could be assigned to a given
violation.
Alternative Public Outreach Methodologies
A review of practices both in Maryland and in other states indicates that there is a wide range of
practices designed to inform the general public about the food safety performance of food service
facilities. Food service facility inspection reports are a matter of public record and as a result a wide
range of strategies have been employed both in Maryland and other states to highlight inspection
findings. These include:
1. Posting of the latest inspection report at a prominent point in the facility.
2. Posting of the latest inspection results on a State or local jurisdiction website.
3. Providing a chronology of inspection results on a State or local jurisdiction website.
4. Posting only the critical violation results on a State or local jurisdiction website.
5. Posting only food service facility closings on a State or local jurisdiction website.
6. Utilizing local media to publicize closings or critical violation results at a food
service facility.
Increasing public outreach by the above methodologies results in two challenges:
● Finding the resources to provide and maintain the public display of information; and
● Providing significant public education as to the significance of the reported
information.

Page 19
Finding 3: Letter Grading of Food Service Facilities
The implementation of letter grading of food service facility inspections does not appear to provide a
useful tool for improving public health safety for the patrons of food service facilities and is likely to
increase the resources committed to regulatory activities without an identifiable benefit.
There is no statewide readily accessible source of food service facility inspection information that
the general public could use to influence their choice of eating facilities.
Recommendation 3: Letter Grading of Food Service Facilities
The Task Force does not recommend adopting any form of Letter Grading or scoring of inspection
reports of food service facilities. The Task Force did consider alternatives to letter grading, and
recommends the following:
Recommendation 4: Alternatives to Letter Grading of Food Service Facilities
The Task Force encourages the routine publication of those parts of facility inspection reports, which
relate to those items, generally known as the critical items, most closely related to public health.
The Task Force had no particular preference for publication method but recognized that publication
of inspection results and maintenance of a website will place a resource burden on the enforcement
organizations which would require additional funds be made available to support this activity in the
interests of public health and transparency.

Page 20
APPENDIX 1: Task Force Membership
Name
Membership Category
Honorable Shawn Tarrant
Maryland House of Delegates
Honorable Jamie Raskin
Member of the Maryland Senate
Alan Brench
Maryland Department of Health and Mental Hygiene (DHMH)
Dr. Cynthia Tucker
Baltimore City Council representative
Susan Thweatt
Prince George’s County Health Department
George Dahlman
Food Allergy Research and Education
Mike Bacharach
Consumer with a food allergy
Marianne Quinn
Parent of a child with a food allergy
Anthony Clarke
Restaurant Owner/Operator (Irish Restaurant Company)
William Weichelt
National Restaurant Association
Keith Sykes
Maryland Retailers Association (Safeway)
Katie Doherty
Maryland Hotel and Lodging Association (ARAMARK Corp.)
Clark Beil
Inter-Jurisdictional Food Service Manager Program Committee
(Montgomery Co.)
Susan Kelly
Maryland Association of County Health Officers (MACHO) (Harford Co.)
Yvonne DeLoatch
Maryland Conference of Local Environmental Health Officers
(Baltimore Co.)

Page 21
APPENDIX 2: Chapter 252 – House Bill 9 (2013 Legislative Session)
HOUSE BILL 9
J1, P1 3lr0725
(PRE–FILED) CF SB 390
By Delegates Hixson, Valderrama, Howard, and Simmons
Requested: November 8, 2012
Introduced and read first time: January 9, 2013
Assigned to: Health and Government Operations
Committee Report: Favorable with amendments
House action: Adopted
Read second time: March 17, 2013
CHAPTER ______
AN ACT concerning
Health – Food Allergy Awareness, Food Safety, and Food Service Facility Letter Grading –
Posting Requirement and Task Force
FOR the purpose of requiring certain food establishments to display, in a certain manner and
location, a certain poster relating to food requiring, on or before a certain date, the
Department of Health and Mental Hygiene, in consultation with certain entities, to create
and make available on its Web site a certain poster; establishing a Task Force to Study
Food Allergy Awareness, Food Safety, and Food Service
Facility Letter Grading; providing for the membership and chair of the Task Force;
authorizing the Task Force to form subcommittees from among its members; requiring the
Department of Health and Mental Hygiene to provide 3 staff for the Task Force; providing
that a member of the Task Force may not 4 receive certain compensation but is entitled to
certain reimbursement; 5 providing for the duties of the Task Force; requiring the Task Force
to report 6 certain findings and recommendations, on or before a certain date, to the 7
Governor and certain committees of the General Assembly; providing for the 8 effective
dates of this Act; providing for the termination of certain provisions of 9 this Act; and
generally relating to food allergy awareness, food safety, and food 10 service facility letter
grading.
BY adding to Article – Health – General Section 21–330.2 Annotated Code of Maryland (2009
Replacement Volume and 2012 Supplement)

Page 22
SECTION 1. BE IT ENACTED BY THE GENERAL ASSEMBLY OF MARYLAND, That the
Laws of Maryland read as follows:
Article – Health – General 21–330.2.
(A) Beginning March 1, 2014, a food establishment shall display prominently in the staff
area 28 of the food establishment a poster relating to food allergy awareness that includes
information regarding the risk of an allergic reaction.
(b) On or before January 1, 2014, the department, in consultation with the restaurant
association of Maryland and food allergy research and education, shall create and make
available on its web site the poster required to be displayed under paragraph (1)(i) of this
subsection (a) of this section.; and
SECTION 2. AND BE IT FURTHER ENACTED, That:
(a) There is a Task Force to Study Food Allergy Awareness, Food Safety, and 17 Food Service
Facility Letter Grading.
(b) The Task Force consists of the following members:
(1) one member of the Senate of Maryland, appointed by the President 20 of the Senate;
(2) one member of the House of Delegates, appointed by the Speaker of 22 the House;
(3) one representative of the Department of Health and Mental Hygiene, appointed by the
Secretary of Health and Mental Hygiene;
(4) the President of the Baltimore City Council, or the President’s 26 designee;
(5) the Prince George’s County Health Officer, or the Health Officer’s 28 designee; and
(6) the following members, appointed by the Governor:
(i) one representative of Food Allergy Research and Education;
(ii) one consumer with a food allergy;
(iii) one parent of a child with a food allergy;
(iv) one representative of the Restaurant Association of Maryland;
(v) one representative of the National Restaurant Association;
(vi) one representative of the Maryland Retailers Association;
(vii) one representative of the Maryland Hotel and Lodging Association;
(viii) one representative of the Inter–Jurisdictional Food Service Manager Program
Committee;
(ix) one representative of the Maryland Association of County Health Officers who is
not from a jurisdiction with a certified food service manager program; and

Page 23
(x) one representative of the Maryland Conference of Local Environmental Health
Directors.
(c) The President of the Senate and Speaker of the House jointly shall designate the chair of the Task
Force.
(d) The Task Force may form subcommittees from among its members.
(e) The Department of Health and Mental Hygiene shall provide staff for the Task Force.
(f) A member of the Task Force:
(1) may not receive compensation as a member of the Task Force; but
(2) is entitled to reimbursement for expenses under the Standard State Travel
Regulations, as provided in the State budget.
(g) The Task Force shall:
(1) study and make recommendations regarding:
(i) food allergy awareness and food allergy training for food service facilities in
the State;
(ii) food safety training for food service facilities in the State; and
(iii) the use of systems for grading and classifying health inspection results for
food service facilities in the State;
(2) review food safety efforts at the State and local level, including:
(i) the frequency of food service facility inspections,
(ii) the most common violations, and the reasons for closures;
(iii) the number of food–borne illness cases that have been linked to food service
facilities; and
(iv) the impact of local food service manager certification programs;
(3) study: the most common food allergies and issues related to
(i) food preparation and cross–contamination in food service facilities;
(ii) existing and planned food allergy training material, programs, and
certifications;
(iii) food allergy awareness and training mandates for food service facilities in
other states;
(iv) legal issues related to food allergens, including potential civil liability,
compliance with the Americans with Disabilities Act, and negligence issues;
(v) the use of grading and classifying health inspection results for food service
facilities by other jurisdictions; the frequency of food–borne illness cases
linked to food service facilities in jurisdictions that grade and classify health

Page 24
inspection results compared to similar jurisdictions that do not use grading
and classification systems;
(vi) the costs of implementing and administering grading and classifying systems,
how the costs of these systems are paid for, and any cost–benefit analyses of
these systems that have been completed;
(vii) the alternatives to grading and classifying health inspection results, including
the State’s existing pass–fail inspection system, online posting of health
inspection results, a system that informs consumers regarding the frequency of
health inspections at food service facilities, and any other options the Task
Force considers appropriate; and
(viii) any other issues the Task Force considers appropriate; and
(4) study and evaluate: mandated food service manager certification and mandated food
handler training options; and online food safety training programs for certification and
recertification.
(h) On or before January 1, 2014, the Task Force shall report its findings and recommendations
related to food allergy awareness and training, food safety training, and the use of grading and
classifying health inspections results for food service facilities to the Governor and, in accordance
with § 2–1246 of the State Government Article, the Senate Finance Committee and the House
Health and Government Operations Committee.
SECTION 3. AND BE IT FURTHER ENACTED, That Section 1 of this Act shall take effect
October 1, 2013.
SECTION 4. AND BE IT FURTHER ENACTED, That, except as provided in Section 3 of this Act,
this Act shall take effect June 1, 2013. Section 2 of this Act shall remain effective for a period of 1
year and 1 month and, at the end of June 30, 2014, with no further action required by the General
Assembly, Section 2 of this Act shall be abrogated and of no further force and effect.

Page 25
APPENDIX 3: Task Force Activity Meetings
The Task force met on an approximately two week time cycle with each meeting comprising of
mixture of subject matter presentations followed by a period of discussion.
Meeting Date.
Time.
Location.
August 15, 2013
10:00 hrs.
Dept. of Transport Headquarters Building
September 12, 2013
14:00 hrs.
Dept. of Transport Headquarters Building
October 3, 2013
13:00 hrs.
Dept. of Transport Headquarters Building
October 17, 2013
9:30 hrs.
House Office Building
November 7, 2013
13:00 hrs.
Dept. of Transport Headquarters Building
November 21, 2013
14:00 hrs.
Dept. of Transport Headquarters Building
December 12, 2013
13:00 hrs.
Dept. of Transport Headquarters Building

Page 26
APPENDIX 4: Overview of Issues Associated with Living with Food Allergies.
(Provided by Food Allergy Research & Education (FARE))
The Physical Impact of Food Allergies
The job of the body’s immune system is to identify and destroy germs (such as bacteria or viruses)
that make you sick. A food allergy results when the immune system mistakenly targets a harmless
food protein – an allergen – as a threat and attacks it.
Unlike other types of food disorders, such as intolerances, food allergies are “IgE mediated.” This
means that your immune system produces abnormally large amounts of an antibody called
immunoglobulin E — IgE for short. IgE antibodies fight the “enemy” food allergens by releasing
histamine and other chemicals, which trigger the symptoms of an allergic reaction.
When an individual with a food allergy is exposed to their allergen, usually by consuming foods
containing the forbidden ingredient, their reactions can range from mild to severe, including the
potentially life-threatening condition known as anaphylaxis. During anaphylaxis, allergic symptoms
can affect several areas of the body and may threaten breathing and blood circulation. A food
allergic reaction may affect an individual’s skin (hives/swelling), the gastrointestinal tract
(diarrhea/discomfort), the respiratory tract (difficulties breathing), and, in the most serious cases, the
cardiovascular system (cardiac arrest).
There is no cure for food allergies and only strict avoidance to even minute quantities of the allergen
will prevent a reaction.
The following facts are vital to understanding food allergies.
Every 3 minutes, a food allergy reaction sends someone to the emergency department –
that is more than 200,000 emergency department visits per year.
The U.S. Centers for Disease Control reported that food allergies result in more than
300,000 ambulatory-care visits a year among children under the age of 18. Food allergy
is the leading cause of anaphylaxis outside the hospital setting.
Food allergy results in approximately 150-200 fatalities per year.
Once an anaphylactic reaction starts, a medication called epinephrine is the first line of
defense to treat the reaction.
Teenagers and young adults with food allergies are at the highest risk of fatal food-
induced anaphylaxis.
Individuals with food allergies who also have asthma may be at increased risk for
severe/fatal food allergy reactions.
Symptoms of anaphylaxis may recur after initially subsiding and experts recommend an
observation period of about four hours to monitor that the reaction has been resolved.
Failure to promptly (i.e., within minutes) treat food anaphylaxis with epinephrine is a risk
factor for fatalities.

Page 27
There is no cure for food allergies. Strict avoidance of food allergens and early
recognition and management of allergic reactions to food are important measures to
prevent serious health consequences.
The Restaurant Setting
Dining in restaurants is especially challenging for food allergic individuals who must constantly
guard themselves against accidental exposure, especially in a venue where food is being prepared by
individuals who are unfamiliar with food allergies. Even trace amounts of the food allergen can
cause a reaction. The situation is especially dangerous in a restaurant setting, where food allergens
can be hidden in menu items, and there is a substantial risk of cross-contact during food preparation
in the kitchen. In fact, a significant number of fatal and near-fatal reactions are triggered by
restaurant food. In two published studies, food service establishments including restaurants were the
cause of fatal food allergic reactions approximately one-third to one half of the time.
Communication and education strategies are the most effective means of reducing the risks of
accidental exposures. In a recent study, 62% of recorded adverse reactions, the restaurant was not
properly notified of the allergy. A clear line of communication between patron, server, and food
preparer can alleviate risk.
Restaurant employees generally receive little or no training on the serious nature of food allergy;
reading ingredient labels; the importance of strict allergen avoidance; and avoiding cross-contact
during food preparation. As a result, restaurant staff often cannot accurately respond to inquiries
from food-allergic customers or help them select safe menu items and may be vastly misinformed.
The wide-spread lack of understanding contributes to the risk of fatal reactions.
Lack of awareness in this area is both prevalent and dangerous. In a survey given to one hundred
restaurant personnel, including managers, chefs, and waitstaff, one-quarter of the respondents
incorrectly indicated that removing an allergen from a finished meal (e.g., taking off nuts) was safe;
and one-quarter incorrectly indicated that consuming a small amount of an allergen would be safe.
This lack of understanding could have life threatening consequences for customers with food
allergies.
Restaurants sensitivity to the needs of individuals with food allergy will address risks. Procedures
to manage food-allergic patrons, personnel training about food allergies, the potential for trace
protein contamination to trigger reactions, methods by which to avoid cross- contact and the means
of activating emergency assistance in the event of a reaction would all minimize risk of life-
threatening reactions.
The lack of education/training can be a key contributor to fatal reactions, and prevents food-allergic
individuals from safely enjoying restaurant meals.

Page 28
The Food Service Industry
The impact of food allergies is both a challenge and opportunity for the food service industry.
According to a survey by the National Restaurant Association, some 87% of restaurants believe food
allergies are extremely important and expect increased attention to it. Yet 43% concede they do not
train their staff on food allergens.
Currently the revenue lost from food allergy families avoiding restaurant dining is estimated at $45
million – a week. However, the global food market for those with food allergies is expected to grow
more than $26.5 billion over the next five years and the increase in revenue by accommodating food
allergic patrons is expected to increase 10-25%, according to the National Restaurant Association.

Page 29
APPENDIX 5: Massachusetts Allergen Law
In response to the law Chapter 10 of Massachusetts State Sanitary Code, 105 CMR (Code of
Massachusetts Regulations) 590.000, Minimum Sanitation Standards for Food Establishments, was
amended to include the following:
Poster – Section 105 CMR 590.009(G)(1) requires food establishment to display an
MDPH-approved poster in the employee work area. MDPH has approved two (2)
versions of the Food Allergy & Anaphylaxis Network: the 2005 version, and the 2009
version. These posters are available at http://www.foodallergy.org/page/restaurant-
poster. If one of these two posters is on display as required, then additional posters may
be displayed also.
Menu Notice – Section 105 CMR 590.009(G)(2) requires all menus and menu boards in
the food establishment to display the words “Before placing your order, please inform
your server if a person in your party has a food allergy”.
Point of Service Notice – Section 105 CMR 590.009(G)(2)(b)2 allows food establishment
to utilize this option in lieu of placing a notice on a menu board. The wording which
describes the size and location of the notice was taken from section 105 CMR 590.009(F)
and should be able to be “read from a distance of five feet”.
Training Certificate – Sections 105 CMR 590.009(G)(3) requires at least one certified
food protection manager in each food service facility establishment by the regulation to
obtain a food allergen awareness training certificate by February 1, 2011. The names and
contact information about vendors who provide these certificate video are available at the
FPP website discussed above.
Based on practical experience the above requirements appear to be achieving the planned impact on
the operations of Massachusetts food service facilities with respect to allergen awareness and a State
report on the implementation of the Act is in preparation. The Act also includes a provision for the
development of a “Food Allergy Friendly (FAF)” designation for restaurants and the publication of a
list of such facilities. To date this has not been accomplished due to practical difficulties in
specifying a FAF restaurant and establishing measurable criteria that could be used to manage
compliance with the FAF designation. It should also be noted that the Massachusetts Law only
specifically refers the “Major Food Allergens” as defined in the current version of the Food Code.
The Massachusetts Law does provide for the following exemptions:
● Public and private schools, educational institutions, summer camps, childcare facilities,
and other child care programs approved to participate in USDA Child Nutrition Programs
are exempt from 105 CMR 590.009(G), with the exception of 105 CMR
590.009(G)(3)(b)2., provided that they have:
○ Written policies and procedures for identifying, documenting, and
accommodating students with food allergies, and
○ Documentation verifying participation in food allergen training recognized by
the Massachusetts Department of Elementary and Secondary Education and
the Massachusetts Department of Public Health.

Page 30
● Food service operations in institutional settings in which food is prepared and/or served
to a specific population (for example, hospitals, nonprofit organizations, Older American
Act Elderly Nutrition programs, and charitable food facilities) that have written
procedures for identifying, documenting, and accommodating their clients with food
allergies are exempt from 105 CMR 590.009(G)(2).
● Temporary food establishments operated by non-profit organizations are exempt from
105 CMR 590.009(G).
Massachusetts FAQs :
http://www.mass.gov/eohhs/docs/dph/environmental/foodsafety/food-allergen-3-reg-faqs.pdf

Page 31
APPENDIX 6: AG’s Letter on Allergen Legal Summary

Page 32

Page 33

Page 34

Page 35
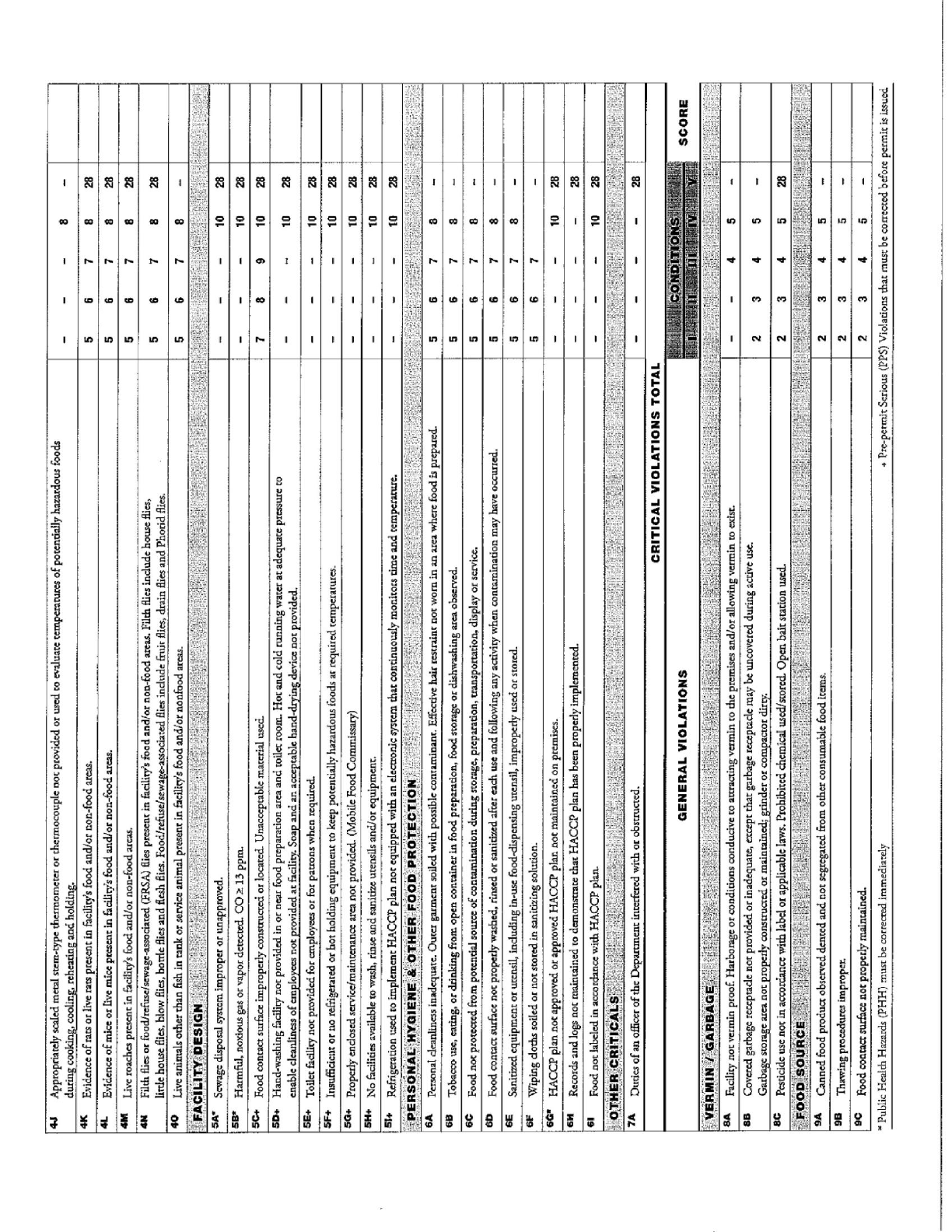
APPENDIX 7: Maryland Food Service Facility Inspection Form

Page 36

Page 37
APPENDIX 8: New York City Food Service Facility Scoring Form

Page 38
Page 39

Page 40

Page 41

Page 42
APPENDIX 9: Los Angeles County Inspection and Scoring Form

Page 43
