
CMS Manual System
Department of Health &
Human Services (DHHS)
Pub. 100-07 State Operations
Provider Certification
Centers for Medicare &
Medicaid Services (CMS)
Transmittal 59
Date: May 21, 2010
SUBJECT: Clarification of the Interpretive Guidelines for the Anesthesia Services
Condition of Participation
I. SUMMARY OF CHANGES: Revisions to Appendix A, “Survey Protocol, Regulations and
Interpretive Guidelines for Hospitals.” This instruction updates and clarifies the guidance for the
Anesthesia Services Condition of Participation and related standards.
NEW/REVISED MATERIAL - EFFECTIVE DATE*: May 21, 2010
IMPLEMENTATION DATE: May 21, 2010
The revision date and transmittal number apply to the red italicized material only. Any other
material was previously published and remains unchanged.
II. CHANGES IN MANUAL INSTRUCTIONS: (N/A if manual not updated.)
(R = REVISED, N = NEW, D = DELETED) – (Only One Per Row.)
R/N/D
CHAPTER/SECTION/SUBSECTION/TITLE
R
Appendix A/§482.52/Condition of Participation Anesthesia Services/
Tag A-1000
R
Appendix A/§482.52(a)/Standard: Organization and Staffing/Tag A-1001
R
Appendix A/§482.52(b)/Standard: Delivery of Services/Tag A-1002
R
Appendix A/§482.52(b)(1)/Standard: Pre-anesthesia Evaluation/Tag A-1003
R
Appendix A/§482.52(b)(2)/Standard: Intraoperative Anesthesia Record/Tag A
1004
R
Appendix A/§482.52(b)(3)/Standard: Post-anesthesia Evaluation/Tag A-1005
III. FUNDING: No additional funding will be provided by CMS; contractor activities are
to be carried out within their operating budgets.
IV. ATTACHMENTS:
Business Requirements
x
Manual Instruction
Confidential Requirements
One-Time Notification
One-Time Notification -Confidential
Recurring Update Notification
*Unless otherwise specified, the effective date is the date of service.

A-1000
(Rev.59, Issued: 05-21-10, Effective/Implementation: 05-21-10)
§482.52 Condition of Participation: Anesthesia Services
If the hospital furnishes anesthesia services, they must be provided in a well-organized
manner under the direction of a qualified doctor of medicine or osteopathy. The service is
responsible for all anesthesia administered in the hospital.
Interpretive Guidelines §482.52
The provision of anesthesia services is an optional hospital service. However, if a hospital
provides any degree of anesthesia service to its patients, the hospital must comply with all the
requirements of this Condition of Participation (CoP).
“Anesthesia” involves the administration of a medication to produce a blunting or loss of:
• pain perception (analgesia);
• voluntary and involuntary movements;
• autonomic function; and
• memory and/or consciousness,
depending on where along the central neuraxial (brain and spinal cord) the medication is
delivered.
In contrast, “analgesia” involves the use of a medication to provide relief of pain through the
blocking of pain receptors in the peripheral and/or central nervous system. The patient does not
lose consciousness, but does not perceive pain to the extent that may otherwise prevail.
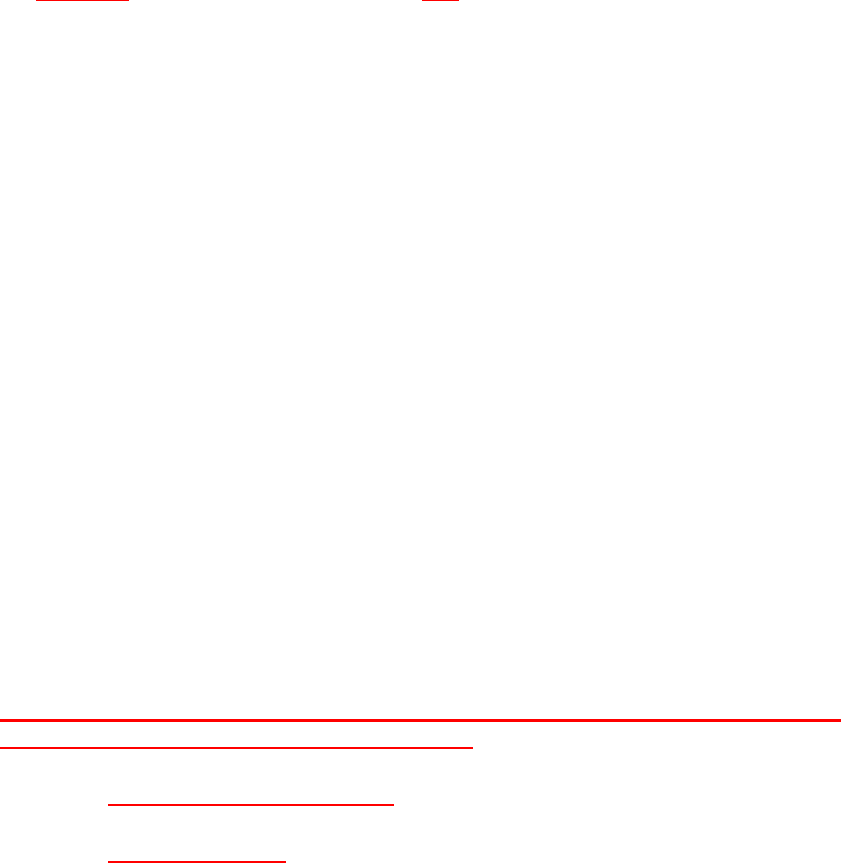
The additional definitions below illustrate differences among the various types of anesthesia
services. Not all of the definitions are considered “anesthesia.” The definitions are generally
based on American Society of Anesthesiologists definitions found in its most recent set of
practice guidelines (Anesthesiology 2002; 96:1004-17). In addition, a visual representation of
these terms is displayed on the next page.
“Anesthesia services” in a hospital subject to the anesthesia administration requirements at 42
CFR 482.52(a):
• General Anesthesia: a drug-induced loss of consciousness during which patients are not
arousable, even by painful stimulation. The ability to independently maintain ventilatory
support is often impaired. Patients often require assistance in maintaining a patent airway,
and positive pressure ventilation may be required because of depressed spontaneous
ventilation or drug-induced depression of neuromuscular function. Cardiovascular function
may be impaired. For example, a patient undergoing major abdominal surgery involving the

No
Hospital
Anesthesia Services
Anesthesia
• General
• Regional
• MAC
• Deep Sedation
Analgesia/Sedation
• Topical
• Local
• Minimal
• Moderate
To be administered
by appropriately
trained medical
practitioner within
scope of practice
To be administered
by anesthesiologist,
qualified physician,
CRNA or anesthesia
assistant as specified
at
§482.52(a)
Rescue Capacity
Opt-Out State?
No MD super-
vision required for
CRNA
MD supervision
required for
CRNA
Yes
Note: analgesia via
epidurals/spinals for Labor
& Delivery is permitted to
be administered by
CRNAs without MD
supervision.
removal of a portion or all of an organ would require general anesthesia in order to tolerate
such an extensive surgical procedure. General anesthesia is used for those procedures when
loss of consciousness is required for the safe and effective delivery of surgical services;
• Regional Anesthesia: the delivery of anesthetic medication at a specific level of the spinal
cord and/or to peripheral nerves, including epidurals and spinals and other central
neuraxial nerve blocks, is used when loss of consciousness is not desired but sufficient
analgesia and loss of voluntary and involuntary movement is required. Given the potential
for the conversion and extension of regional to general anesthesia in certain procedures, it is
necessary that the administration of regional and general anesthesia be delivered or
supervised by a practitioner as specified at 42 CFR 482.52(a).
The administration of medication via an epidural or spinal route for the purpose of
analgesia, during labor and delivery, is not considered anesthesia and therefore is not
subject to the anesthesia supervision requirements at 42 CFR 482.52(a). However, if the
obstetrician or other qualified physician attending to the patient determines that an operative
delivery (i.e., C-section) of the infant is necessary, it is likely that the subsequent
administration of medication is for anesthesia, as defined above, and the anesthesia
supervision requirements at 42 CFR 482.52(a) would apply.
• Monitored Anesthesia Care (MAC): anesthesia care that includes the monitoring of the
patient by a practitioner who is qualified to administer anesthesia as defined by the
regulations at §482.52(a). Indications for MAC depend on the nature of the procedure, the
patient’s clinical condition, and/or the potential need to convert to a general or regional
anesthetic. Deep sedation/analgesia is included in MAC.
- Deep sedation/analgesia: a drug-induced depression of consciousness during which
patients cannot be easily aroused but respond purposefully following repeated or
painful stimulation. The ability to independently maintain ventilatory function may
be impaired. Patients may require assistance in maintaining a patent airway, and
spontaneous ventilation may be inadequate. Cardiovascular function is usually
maintained. An example of deep sedation would be a screening colonoscopy when
there is a decision to use propofol, so as to decrease movement and improve
visualization for this type of invasive procedure. Because of the potential for the
inadvertent progression to general anesthesia in certain procedures, it is necessary
that the administration of deep sedation/analgesia be delivered or supervised by a
practitioner as specified in 42 CFR 482.52(a).
“Anesthesia services” in a hospital NOT subject to the anesthesia administration and
supervision requirements at 42 CFR 482.52(a):
• Topical or Local Anesthesia;
• Minimal Sedation: A drug-induced state during which patients respond normally to
verbal commands. Although cognitive function and coordination may be impaired,
ventilator and cardiovascular functions are unaffected. For example, a patient
undergoing an MRI or CT scan may receive minimal sedation with an oral

medication to decrease the anxiety while undergoing these types of radiologic
examinations;
• Moderate Sedation/Analgesia: (“Conscious Sedation”): A drug-induced depression
of consciousness during which patients respond purposefully to verbal commands,
either alone or accompanied by light tactile stimulation. No interventions are
required to maintain a patent airway, and spontaneous ventilation is adequate.
Cardiovascular function is usually maintained. For example, a patient undergoing
the reduction of a dislocated large joint (shoulder) may require this form of sedation
to tolerate the procedure.
• Rescue Capacity. Because sedation is a continuum, it is not always possible to
predict how an individual patient will respond. Hence, hospitals must ensure that
procedures are in place to rescue patients whose level of sedation becomes deeper
than initially intended, for example, patients who inadvertently enter a state of Deep
Sedation/Analgesia when moderate sedation was intended. “Rescue” from a deeper
level of sedation than intended requires an intervention by a practitioner with
expertise in airway management and advanced life support. The qualified
practitioner corrects the adverse physiologic consequences of the deeper-than-
intended level of sedation and returns the patient to the originally intended level of
sedation.
Anesthesia services throughout the hospital (including all departments in all campuses and off-
site locations where anesthesia services are provided) must be organized into one anesthesia
service, under the direction of a qualified doctor of medicine (MD) or doctor of osteopathy
(DO). Areas where anesthesia services are furnished may include (but are not limited to):
• Operating room suite(s), both inpatient and outpatient;
• Obstetrical suite(s);
• Radiology department;
• Clinics;
• Emergency department;
• Psychiatry department;
• Outpatient surgery areas; and
• Special procedures area (e.g., endoscopy suite, pain management clinic, etc.).
The hospital’s medical staff establishes criteria for the qualifications for the director of the
anesthesia services in accordance with State laws and acceptable standards of practice. The
anesthesia service is responsible for developing policies and procedures governing the provision
of all categories of anesthesia services, including specifying the minimum qualifications for each
category of practitioner who is permitted to provide anesthesia services that are not subject to
the anesthesia administration requirements at 42 CFR 482.52(a).
A well-organized anesthesia service must be integrated into the hospital’s required Quality
Assessment/Performance Improvement program, in order to assure the provision of safe care to
patients.
Survey Procedures §482.52
• Request a copy of the organizational chart for anesthesia services.
• Determine that a doctor of medicine or osteopathy has the authority and responsibility for
directing the administration of all anesthesia throughout the hospital.
• Look for evidence of the director’s appointment. Review the position description.
Confirm that the director’s responsibilities include at least the following:
- Planning, directing, and supervising all activities of the service;
- Establishing staffing schedules;
- Evaluating the quality and appropriateness of the anesthesia patient care;
• Review the hospital’s anesthesia policies and procedures.
- Do they address who may provide anesthesia services in each setting where such
services are furnished, and are these policies in compliance with the regulations?
- Do they apply in all hospital locations where anesthesia services are provided?
______________________________________________________________________________
A-1001
(Rev.59, Issued: 05-21-10, Effective/Implementation: 05-21-10)
§482.52(a) Standard: Organization and Staffing
The organization of anesthesia services must be appropriate to the scope of the services
offered. Anesthesia must be administered only by --
(1) A qualified anesthesiologist;
(2) A doctor of medicine or osteopathy (other than an anesthesiologist);
(3) A dentist, oral surgeon, or podiatrist who is qualified to administer anesthesia
under State law;

(4) A certified registered nurse anesthetist (CRNA), as defined in §410.69(b) of this
chapter, who, unless exempted in accordance with paragraph (c) of this section, is
under the supervision of the operating practitioner or of an anesthesiologist who is
immediately available if needed; or
(5) An anesthesiologist’s assistant, as defined in Sec. 410.69(b) of this chapter, who is
under the supervision of an anesthesiologist who is immediately available if
needed.
§482.52(c) Standard: State Exemption
(1) A hospital may be exempted from the requirement for MD/DO supervision of
CRNAs as described in paragraph (a)(4) of this section, if the State in which the
hospital is located submits a letter to CMS signed by the Governor, following
consultation with the State’s Boards of Medicine and Nursing, requesting
exemption from MD/DO supervision of CRNAs. The letter from the Governor
must attest that he or she has consulted with State Boards of Medicine and
Nursing about issues related to access to and the quality of anesthesia services in
the State and has concluded that it is in the best interests of the State’s citizens to
opt-out of the current MD/DO supervision requirement, and that the opt-out is
consistent with State law.
(2) The request for exemption and recognition of State laws, and the withdrawal of
the request may be submitted at any time, and are effective upon submission.
Interpretive Guidelines §482.52(a) and (c)
Who May Administer Anesthesia
Topical/local anesthetics, minimal sedation, moderate sedation
The requirements at §482.52(a) concerning who may administer anesthesia do not apply to the
administration of topical or local anesthetics, minimal sedation, or moderate sedation.
However, the hospital must have policies and procedures, consistent with State scope of practice
law, governing the provision of these types of anesthesia services. Further, hospitals must
assure that all anesthesia services are provided in a safe, well-organized manner by qualified
personnel.
General anesthesia, regional anesthesia and monitored anesthesia, including deep
sedation/analgesia, may only be administered by:
• A qualified anesthesiologist;
• An MD or DO (other than an anesthesiologist);
• A dentist, oral surgeon or podiatrist who is qualified to administer anesthesia under State
law;
• A CRNA who is supervised by the operating practitioner or by an anesthesiologist who is
immediately available if needed; or

• An anesthesiologist’s assistant under the supervision of an anesthesiologist who is
immediately available if needed.
Administration by an MD/DO/dentist/oral surgeon/podiatrist
The hospital’s anesthesia services policies must address the circumstances under which an MD
or DO who is not an anesthesiologist, a dentist, oral surgeon or podiatrist is permitted to
administer anesthesia. In the case of a dentist, oral surgeon or podiatrist, administration of
anesthesia must be permissible under State law and comply with all State requirements
concerning qualifications. Hospitals should conform to generally accepted standards of
anesthesia care when establishing policies governing anesthesia administration by these types of
practitioners as well as MDs or DOs who are not anesthesiologists.
Administration by a CRNA
Unless the hospital is located in a State that has chosen to opt out of the CRNA supervision
requirements, a CRNA administering general, regional and monitored anesthesia must be
supervised either by the operating practitioner who is performing the procedure, or by an
anesthesiologist who is immediately available.
Hospitals should conform to generally accepted standards of anesthesia care when establishing
policies for supervision by the operating practitioner. An anesthesiologist is considered
“immediately available” when needed by a CRNA under the anesthesiologist’s supervision only
if he/she is physically located within the same area as the CRNA, e.g., in the same operative/
procedural suite, or in the same labor and delivery unit, and not otherwise occupied in a way
that prevents him/her from immediately conducting hands-on intervention, if needed.
If the hospital is located in a State where the Governor has submitted a letter to CMS attesting
that he or she has consulted with State Boards of Medicine and Nursing about issues related to
access to and the quality of anesthesia services in the State and has concluded that it is in the
best interests of the State’s citizens to opt-out of the current physician supervision requirement,
and that the opt-out is consistent with State law, then a hospital may permit a CRNA to
administer anesthesia without operating practitioner or anesthesiologist supervision. (A list of
States that have opted out of the CRNA supervision requirement may be found at
http://www.cms.hhs.gov/CFCsAndCoPs/02_Spotlight.asp)
A CRNA is defined in §410.69(b) as a “registered nurse who:
(1) Is licensed as a registered professional nurse by the State in which the nurse
practices;
(2) Meets any licensure requirements the State imposes with respect to non-physician
anesthetists;
(3) Has graduated from a nurse anesthesia educational program that meets the
standards of the Council on Accreditation of Nurse Anesthesia Programs, or such
other accreditation organization as may be designated by the Secretary; and
(4) Meets the following criteria:
(i) Has passed a certification examination of the Council on Certification of
Nurse Anesthetists, the Council on Recertification of Nurse Anesthetists, or
any other certification organization that may be designated by the Secretary;
or
(ii) Is a graduate of a program described in paragraph (3) of this definition and
within 24 months after that graduation meets the requirements of paragraph
(4)(i) of this definition.”
Administration by an Anesthesiologist’s Assistant
An anesthesiologist’s assistant may administer anesthesia when under the supervision of an
anesthesiologist. The anesthesiologist must be immediately available if needed. An
anesthesiologist is considered “immediately available” to assist the anesthesiologist’s assistant
under the anesthesiologist’s supervision only if he/she is physically located within the same area
as the anesthesiologist’s assistant, e.g., in the same operative/procedural suite, or in the same
labor and delivery unit, and not otherwise occupied in a way that prevents him/her from
immediately conducting hands-on intervention, if needed.
An anesthesiologist’s assistant is defined at §410.69(b) as a “person who-
(1) Works under the direction of an anesthesiologist;
(2) Is in compliance with all applicable requirements of State law, including any
licensure requirements the State imposes on nonphysician anesthetists; and
(3) Is a graduate of a medical school-based anesthesiologist’s assistant education
program that –
(a) Is accredited by the Committee on Allied Health Education and Accreditation;
and
(b) Includes approximately two years of specialized basic science and clinical
education in anesthesia at a level that builds on a premedical undergraduate
science background.”
Anesthesia Services Policies
The medical staff bylaws or rules and regulations must include criteria for determining the
anesthesia service privileges to be granted to an individual practitioner and a procedure for
applying the criteria to individuals requesting privileges, as required by the regulations at §482.
22(c)(6) for any type of anesthesia services, including those not subject to the anesthesia
administration requirements at §482.52(a). The hospital’s governing body must approve the
specific anesthesia service privileges for each practitioner who furnishes anesthesia services,
addressing the type of supervision, if any, required. The privileges granted must be in
accordance with State law and hospital policy. The type and complexity of procedures for which
the practitioner may administer anesthesia must be specified in the privileges granted to the
individual practitioner. Deficiencies related to these requirements should be cited under §482.
22(c)(6).
When a hospital permits operating practitioners to supervise a CRNA administering anesthesia,
the medical staff bylaws or rules and regulations must specify for each category of operating
practitioner, the type and complexity of procedures that category of practitioner may supervise.
However, individual operating practitioners do not need to be granted specific privileges to
supervise a CRNA.
Survey Procedures §482.52(a) and (c)
• Review the qualifications of individuals authorized to administer general anesthesia,
regional anesthesia and monitored anesthesia, including deep sedation/analgesia to
determine if they satisfy the requirements at §482.52(a) and (c).
• Determine that there is documentation of current licensure and, as applicable, current
certification for all persons administering anesthesia.
• Determine if the state is an “opt-out state” and therefore permits CRNAs to administer
anesthesia without supervision in accordance with 482.52(c).
• Review the hospital’s policies and procedures governing supervision of CRNA’s and
anesthesiologist’s assistants, and determine whether they comply with the regulatory
requirements. and
• Review the qualifications of individuals authorized to furnish other anesthesia services,
to determine if they are consistent with the hospital’s anesthesia service policies.
_____________________________________________________________________________
A-1002
(Rev.59, Issued: 05-21-10, Effective/Implementation: 05-21-10)
§482.52(b) Standard: Delivery of Services
Anesthesia services must be consistent with needs and resources. Policies on anesthesia
procedures must include the delineation of preanesthesia and postanesthesia
responsibilities. The policies must ensure that the following are provided for each patient:
Interpretive Guidelines §482.52(b)
Anesthesia services must be delivered in a manner that is consistent with the needs and the
resources of the hospital. Anesthesia policies at a minimum must address:
• How the hospital’s anesthesia services needs will be met;
• Delivery of anesthesia services consistent with recognized standards for anesthesia care.
A well-designed anesthesia services policy would address issues such as:
• Patient consent;
• Infection control measures;
• Safety practices in all anesthetizing areas;
• Protocol for supportive life functions, e.g., cardiac and respiratory emergencies;
• Reporting requirements;
• Documentation requirements;
• Equipment requirements, as well as the monitoring, inspection, testing, and
maintenance of anesthesia equipment in the hospital’s biomedical equipment
program.
• Delineation of pre- and post-anesthesia staff responsibilities
Survey Procedures §482.52(b)
Review the policies developed on anesthesia procedures. Determine whether the anesthesia
service policies for delivery of care address the issues identified in interpretive guidelines.
________________________________________________________________________
A-1003
(Rev.59, Issued: 05-21-10, Effective/Implementation: 05-21-10)
[The policies must ensure that the following are provided for each patient:]
§482.52(b) (1) - A pre-anesthesia evaluation completed and documented by an individual
qualified to administer anesthesia, as specified in paragraph (a) of this section, performed
within 48 hours prior to surgery or a procedure requiring anesthesia services.
Interpretive Guidelines §482.52(b)(1)
A pre-anesthesia evaluation must be performed for each patient who receives general, regional
or monitored anesthesia. While current practice dictates that the patient receiving moderate
sedation be monitored and evaluated before, during, and after the procedure by trained
practitioners, a pre-anesthesia evaluation is not required because moderate sedation is not
considered to be “anesthesia”, and thus is not subject to this requirement.
The evaluation must be performed by someone qualified to administer anesthesia as specified in
§482.52(a), i.e., only by:
• A qualified anesthesiologist;
• A doctor of medicine or osteopathy (other than an anesthesiologist);
• A dentist, oral surgeon, or podiatrist who is qualified to administer anesthesia under
State law;
• A certified registered nurse anesthetist (CRNA), who, unless exempted in accordance
with paragraph (c) of this section, is under the supervision of the operating practitioner
or of an anesthesiologist who is immediately available if needed; or
• An anesthesiologist’s assistant who is under the supervision of an anesthesiologist who is
immediately available if needed.
Although §482.12 (c)(1)(i) provides broad authority to physicians to delegate tasks to other
qualified medical personnel, the more stringent requirements at §482.52(b)(1) do not permit
delegation of the pre-anesthesia evaluation to practitioners who are not qualified to administer
anesthesia.
The pre-anesthesia evaluation must be performed within 48 hours prior to any inpatient or
outpatient surgery or procedure requiring anesthesia services. The delivery of the first dose of
medication(s) for the purpose of inducing anesthesia, as defined above, marks the end of the 48
hour time frame.
In accordance with current standards of anesthesia care, the pre-anesthesia evaluation of the
patient includes, at a minimum:
• Review of the medical history, including anesthesia, drug and allergy history;
• Interview and examination of the patient;
• Notation of anesthesia risk according to established standards of practice (e.g., ASA
classification of risk);
• Identification of potential anesthesia problems, particularly those that may suggest
potential complications or contraindications to the planned procedure (e.g., difficult
airway, ongoing infection, limited intravascular access);
• Additional pre-anesthesia evaluation, if applicable and as required in accordance with
standard practice prior to administering anesthesia (e.g., stress tests, additional
specialist consultation);
• Development of the plan for the patient’s anesthesia care, including the type of
medications for induction, maintenance and post-operative care and discussion with the
patient (or patient’s representative) of the risks and benefits of the delivery of anesthesia.
Survey Procedures §482.52(b)(1)
• Review a sample of inpatient and outpatient medical records for patients who had surgery
or a procedure requiring administration of anesthesia.
• Determine whether each patient had a pre-anesthesia evaluation by a practitioner
qualified to administer anesthesia.
• Determine whether each patient’s pre-anesthesia evaluation included at least the
elements described above.
• Determine that the pre-anesthesia evaluation was performed within 48 hours prior to the
delivery of the first dose of medication(s) given for the purpose of inducing anesthesia for
the surgery or a procedure requiring anesthesia services.
_____________________________________________________________________________
A-1004
(Rev.59, Issued: 05-21-10, Effective/Implementation: 05-21-10)
[The policies must ensure that the following are provided for each patient:]
§482.52(b)(2) - An intraoperative anesthesia record.
Interpretive Guidelines §482.52(b)(2)
There must be an intraoperative anesthesia record or report for each patient who receives
general, regional or monitored anesthesia. While current practice dictates that the patient
receiving moderate sedation be monitored and evaluated before, during, and after the procedure
by trained practitioners, an intraoperative anesthesia report is not required because, as
explained above , moderate sedation is not “anesthesia”. Current standard of care stipulates
that an intraoperative anesthesia record, at a minimum, includes:
• Name and hospital identification number of the patient;
• Name(s) of practitioner(s) who administered anesthesia, and as applicable, the name and
profession of the supervising anesthesiologist or operating practitioner;
• Name, dosage, route and time of administration of drugs and anesthesia agents;
• Techniques(s) used and patient position(s), including the insertion/use of any
intravascular or airway devices;
• Name and amounts of IV fluids, including blood or blood products if applicable;
• Timed-based documentation of vital signs as well as oxygenation and ventilation
parameters; and
• Any complications, adverse reactions, or problems occurring during anesthesia,
including time and description of symptoms, vital signs, treatments rendered, and
patient’s response to treatment.
Survey Procedures §482.52(b)(2)
Review records to determine that each patient has an intraoperative anesthesia record that
includes the elements described above.
______________________________________________________________________
A-1005
(Rev.59, Issued: 05-21-10, Effective/Implementation: 05-21-10)
[The policies must ensure that the following are provided for each patient:]
482.52(b)(3) - A postanesthesia evaluation completed and documented by an individual
qualified to administer anesthesia, as specified in paragraph (a) of this section, no later
than 48 hours after surgery or a procedure requiring anesthesia services. The
postanesthesia evaluation for anesthesia recovery must be completed in accordance with
State law and with hospital policies and procedures that have been approved by the
medical staff and that reflect current standards of anesthesia care.
Interpretive Guidelines §482.52(b)(3)
A postanesthesia evaluation must be completed and documented no later than 48 hours after
surgery or a procedure requiring anesthesia services. The evaluation is required any time
general, regional, or monitored anesthesia has been administered to the patient. While current
practice dictates that the patient receiving moderate (conscious) sedation be monitored and
evaluated before, during, and after the procedure by trained practitioners, a postanesthesia
evaluation is not required (71 FR 68691)
The evaluation must be completed and documented by any practitioner who is qualified to
administer anesthesia. In accordance with §482.52(a), anesthesia must be administered only by:
• A qualified anesthesiologist;
• A doctor of medicine or osteopathy (other than an anesthesiologist);
• A dentist, oral surgeon, or podiatrist who is qualified to administer anesthesia under
State law;
• A certified registered nurse anesthetist (CRNA), who, unless exempted in accordance
with paragraph (c) of this section, is under the supervision of the operating practitioner
or of an anesthesiologist who is immediately available if needed; or
• An anesthesiologist’s assistant who is under the supervision of an anesthesiologist who
is immediately available if needed.
Although §482.12(c)(1)(i) provides broad authority to physicians to delegate tasks to other
qualified medical personnel, the more stringent requirements of §482.52(b)(3) do not permit
delegation of the postanesthesia evaluation to practitioners who are not qualified to administer
anesthesia.
The calculation of the 48-hour time frame begins at the point the patient is moved into the
designated recovery area. Except in cases where post-operative sedation is necessary for the
optimum medical care of the patient (e.g., ICU), the evaluation generally would not be
performed immediately at the point of movement from the operative area to the designated
recovery area. Accepted standards of anesthesia care indicate that the evaluation may not begin
until the patient is sufficiently recovered from the acute administration of the anesthesia so as to
participate in the evaluation, e.g., answer questions appropriately, perform simple tasks, etc.
The evaluation can occur in the PACU/ICU or other designated recovery location. The elements
of an adequate post-anesthesia evaluation should be clearly documented and conform to current
standards of anesthesia care, including:
• Respiratory function, including respiratory rate, airway patency, and oxygen saturation;
• Cardiovascular function, including pulse rate and blood pressure;
• Mental status;
• Temperature;
• Pain;
• Nausea and vomiting; and
• Postoperative hydration.
Depending on the specific surgery or procedure performed, additional types of monitoring and
assessment may be necessary.
Survey Procedures §482.52(b)(3)
• Review a sample of medical records for patients who had surgery or a procedure
requiring general, regional or monitored anesthesia to determine whether a post
anesthesia evaluation was written for each patient.
• Determine whether the evaluation was conducted by a practitioner who is qualified to
administer anesthesia.
• Determine whether the evaluation was performed within 48 hours after the surgery or
procedure.
• Determine whether the appropriate elements of a post anesthesia evaluation are
documented in the medical record.
