VOLUME 10 · SPECIAL ISSUE · JANUARY 2020
JOURNAL
OF
NURSING
REGULATION
THE OFFICIAL JOURNAL OF THE NATIONAL COUNCIL OF STATE BOARDS OF NURSING
Advancing Nursing Excellence for Public Protection
A Global Prole
of Nursing Regulation,
Education, and Practice
National Council of State Boards of Nursing
JOURNAL OF NURSING REGULATION Volume 10 • Special Issue • January 2020 Pages 1–116

JOURNAL
OF
NURSING
REGULATION
Official publication of the National Council
of State Boards of Nursing
E--C
Maryann Alexander, PhD, RN, FAAN
Chief Officer, Nursing Regulation
National Council of State Boards of Nursing
Chicago, Illinois
C E O
David C. Benton, RGN, PhD, FFNF, FRCN,
FAAN
R E
Allison Squires, PhD, RN, FAAN
Brendan Martin, PhD
NCSBN B D
President
Julia George, MSN, RN, FRE
President-elect
Jim Cleghorn, MA
Treasurer
Adrian Guerrero, CPM
Area I Director
Cynthia LaBonde, MN, RN
Area II Director
Lori Scheidt, MBA-HCM
Area III Director
Jay P. Douglas, MSM, RN, CSAC, FRE
Area IV Director
Valerie J. Fuller, PhD, DNP, AGACNP-BC,
FNP-BC, FAANP, FNAP
Director-at-Large
Elizabeth Lund, MSN, RN
Director-at-Large
Cathy Borris-Hale, RN, MHA
Director-at-Large
Mark Majek, MA, PHR, SHRM-CP
Director-at-Large
Anne Coghlan, MScN, RN
The Journal of Nursing Regulation is a quarterly, peer-reviewed
professional journal published by Elsevier and supported by the National
Council of State Boards of Nursing (NCSBN), a not-for-profit
organization. NCSBN can be contacted at:
111 East Wacker Drive, Suite 2900
Chicago, IL 60601-4277
Telephone: 1-312-525-3600
Fax: 1-312-279-1032
https://www.ncsbn.org
Copyright © 2020. Produced and printed in the USA. All rights reserved.
No part of this publication may be reproduced or transmitted in any
form, whole or in part, without the permission of the copyright holder,
the National Council of State Boards of Nursing.
Disclaimer
The Journal of Nursing Regulation is a peer-reviewed journal.
Statements, views, and opinions are solely those of the authors and
persons quoted. Such views do not necessarily reflect those of the
publisher. The publisher disclaims all responsibility for any errors or
any injuries to persons or properties resulting from the use of information
or advertisements contained in the journal.
Subscription, advertising, reprints
Go to www.journalofnursingregulation.com or [email protected].
ISSN 2155-8256
E A B
Mohammed Arsiwala, MD
President
Michigan Urgent Care
Livonia, Michigan
Kathy Bettinardi-Angres,
APN-BC, MS, RN, CADC
Professional Assessment Coordinator,
Positive Sobriety Institute
Adjunct Faculty, Rush University
Department of Nursing
Chicago, Illinois
Shirley A. Brekken, MS, RN, FAAN
Executive Director
Minnesota Board of Nursing
Minneapolis, Minnesota
Nancy J. Brent, MS, JD, RN
Attorney At Law
Wilmette, Illinois
Sean Clarke, RN, PhD, FAAN
Executive Vice Dean and Professor
NYU Rory Meyers College of Nursing
New York, New York
Anne Coghlan, MScN, RN
Executive Director and Chief
Executive Officer
College of Nurses of Ontario
Toronto, Ontario, Canada
Sandra Evans, MA, Ed, RN
Emeritus Board Member
National Council of State Boards of Nursing
Boise, Idaho
Suzanne Feetham, PhD, RN, FAAN
Nursing Research Consultant
Children’s National Health System
Washington, DC
Patty Knecht, PhD, RN, ANEF
Vice President, Integration Services
ATI Nursing Education/Ascend Learning
Leawood, Kansas
MT Meadows, DNP, RN, MS, MBA
Director of Professional Practice, AONE
Executive Director, AONE Foundation
Chicago, Illinois
Paula R. Meyer, MSN, RN
Executive Director
Washington State Department of
Health Nursing Care Quality
Assurance Commission
Olympia, Washington
Barbara Morvant, MN, RN
Regulatory Policy Consultant
Baton Rouge, Louisiana
Ann L. O’Sullivan, PhD, CRNP, FAAN
Professor of Primary Care Nursing
Dr. Hildegarde Reynolds Endowed Term
Professor of Primary Care Nursing
University of Pennsylvania
Philadelphia, Pennsylvania
Pamela J. Para, RN, MPH,
CPHRM, ARM, DFASHRM
Risk and Regulatory Specialist
Chicago, Illinois
Carolyn Reed, RN, MA, FCNA
Chief Executive/Registrar
Nursing Council of New Zealand
Wellington, New Zealand
Carol A. Romano, PhD, RN,
FACMI, FAAN
Dean and Professor
Uniformed Services University of the
Health Sciences, Daniel K. Inouye
Graduate School of Nursing
Bethesda, Maryland
Linda R. Rounds, PhD, RN, FNP, FAANP
Professor/Betty Lee Evans Distinguished
Professor of Nursing University of Texas
Medical Branch School of Nursing
Galveston, Texas

Special Issue
A Global Prole
of Nursing Regulation,
Education, and Practice
National Council of State Boards of Nursing

2 Journal of Nursing Regulation
CONTENTS
J • V • S I
Advancing nursing excellence
for public protection
Mission
The Journal of Nursing Regulation provides a
worldwide forum for sharing research,
evidence-based practice, and innovative
strategies and solutions related to nursing
regulation, with the ultimate goal of
safeguarding the public. The journal
maintains and promotes National Council
of State Boards of Nursing’s (NCSBN’s)
values of integrity, accountability, quality,
vision, and collaboration in meeting readers’
knowledge needs.
Manuscript Information
The Journal of Nursing Regulation accepts
timely articles that may advance the science
of nursing regulation, promote the mission
and vision of NCSBN, and enhance com-
munication and collaboration among nurse
regulators, educators, practitioners, and the
scientific community. Manuscripts must be
original and must not have been nor will be
submitted elsewhere for publication. See
www.journalofnursingregulaton.com for
author guidelines and manuscript submis-
sion information.
Letters to the Editor
Send to Maryann Alexander at
malexa[email protected].
A Global Profile of Nursing Regulation, Education, and Practice . . . . . . . . . . .3
The Global Regulatory Atlas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Data Collection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Global View of Regulatory Atlas Data . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Regulation and Governance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
Nursing Regulatory Bodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
NRB Mandates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Composition and Qualifications of NRB . . . . . . . . . . . . . . . . . . . . . . . .6
Licensure and Registration Requirements to Practice . . . . . . . . . . . . . . . . . . .8
Authorization to Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Fitness to Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
National Examination Requirements . . . . . . . . . . . . . . . . . . . . . . . . . .9
Nurse Mobility: Compacts and Mutual Agreements . . . . . . . . . . . . . . . . 11
Nurse Types and Titles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
Other Titles, Roles, and Responsibilities . . . . . . . . . . . . . . . . . . . . . . . 13
Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Nursing Program Approval . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Continuing Competence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Discipline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
Regional View of the GlobalRegulatoryAtlas Data . . . . . . . . . . . . . . . . . . . 19
Africa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
The Americas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Canada . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
The Caribbean Community (CARICOM) . . . . . . . . . . . . . . . . . . . . . . . . . . 28
CARICOM Member States . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28
Associate Member States . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30
Non-CARICOM Nations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Central America . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .33
Mexico . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .34
South America . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
The United States of America . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38
Asia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
China and East Asia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .41
Central Asia and India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Southeast Asia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Australia and Oceania . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Europe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
Eastern Europe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .53
Nordic Region . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
Western and Central Europe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
The Middle East . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Appendix A: Glossary of Terms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
Appendix B: Jurisdictions Not Included in Data Analysis . . . . . . . . . . . . . . . 66
Appendix C: Educational Requirements for Entry into Nursing Programs
by Regions
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
Africa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
The Americas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
Asia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
Australia and Oceania . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
Europe . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Middle East . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 109
Appendix D: Global Regulatory Atlas Questionnaire . . . . . . . . . . . . . . . . . 112

www.journalofnursingregulation.com 3Volume 10
•
Special Issue
•
January 2020
A Global Profile of Nursing Regulation,
Education, and Practice
Keywords: Nursing regulation, nursing education and practice, nursing regulation worldwide, Global Regulatory Atlas
From its inception, nursing has been a global profession. Nurses have cared for patients in their respective countries and traversed the
planet to provide care where needed. The World Health Organization (WHO) has designated 2020—the bicentennial of Florence
Nightingale’s birth—as the “Year of the Nurse and Midwife.” Nightingale embodied the cosmopolitanism that still infuses the nursing
profession. By the age of 34 years, Florence was internationally famous for her service in Turkey as part of the British Army’s employ
-
ment of female nurses during the Crimean War. Nightingale and her fellow nurses practiced in the crosshairs of this flashpoint far
beyond the confines of Victorian society traditionally placed on women and introduced hospital reforms and regulations. As we reflect
on the 200 years that elapsed since the advent of modern nursing, the National Council of State Boards of Nursing (NCSBN) reaffirms
its commitment to regulatory excellence by forging the Global Profile of Nursing Regulation, Education, and Practice, an innovative
initiative for information sharing and data collection among nurse regulators worldwide.
The Global Regulatory Atlas
In fall 2016, NCSBN hosted the landmark Regulation 2030 Conference. Regulation 2030 brought together nursing regulators and lead-
ers from eight countries, nursing professional organizations, the Federation of State Medical Boards, the U.S. Federal Trade Commission,
the Organization of Economic Cooperation and Development, and other groups. These attendees were tasked with mapping the future
of nursing regulation in the following categories: (a) governance, (b) processes, (c) licensure and registration, (d) workforce, (e) education,
(f) fitness for practice, and (g) technology.
The Regulation 2030 Conference identified data, collaboration, and standardization as major thematic requirements that would
enable the evolution of nursing regulation. Specifically, participants imagined the harmonization of regulatory processes around the
world, including the optimized capture and sharing of data across nations and continents.
As a step toward future outcomes, and keeping with the recognition of data sharing, collaboration, and standardization as keys to
delivering those outcomes, NCSBN determined that there was no efficient method for comparing the governance and processes by which
nurses are regulated around the world. Therefore, a single resource containing data on the state of nursing regulation in each country
that was digital, searchable, and allowed easy comparison across jurisdictions was needed. This resource ultimately became known as the
Global Regulatory Atlas. This special issue, “Global Profile of Nursing Regulation, Education, and Practice,” summarizes the rich data
contained within Global Regulatory Atlas into an enlightening anthology that captures the similarities, differences and details of nursing
around the world. A Glossary of frequently used terms in the Atlas and in this report is included in Appendix A.
This data is presented in two parts. Part I reports data and findings from a global perspective. Part II reports this data from a
regional perspective. Note that some jurisdictions or regions do not have data listed in every category for various reasons, including that the data were
not available or collected and documented in their region.
Data Collection
The data and findings in this special issue are based on data collected while developing the Global Regulatory Atlas. Between November
2017 and February 2019, data were compiled from the following 320 jurisdictions:
⦁
12 Canadian provinces and territories (the Northwest territories and Nunavut share a regulatory body and are treated as a single
entity in this profile)
⦁
56 United States (including 50 states, 5 territories, and the District of Columbia)
⦁
Mexico
⦁
5 Central American nations
⦁
24 Caribbean jurisdictions
⦁
36 South American jurisdictions (including Brazil’s 26 states and its Federal District)
⦁
7 Nordic countries
⦁
22 Western and Central European nations

4 Journal of Nursing Regulation
⦁
18 Eastern European countries
⦁
17 Middle Eastern nations
⦁
43 African countries
⦁
37 India (including 28 states and 9 territories, some governed jointly)
⦁
10 Central Asian nations
⦁
6 China and 5 other East Asian nations
⦁
11 Southeast Asian countries
⦁
15 Australia and 14 other nations in Oceania
1
If jurisdictions or subjurisdictions were not counted in the numbers above, it is because they are regulated as part of another
jurisdiction or insufficient data were available for analysis (Appendix B).
A 43-item questionnaire was developed and sent to the above 320 jurisdictions worldwide, covering subject matter such as the
composition of the jurisdiction’s nursing regulatory body, the nursing registry, the different types of nurses the jurisdiction recognizes,
the process for becoming authorized to practice (or continue practicing), nursing education, and the disciplinary process. The complete
questionnaire can be found in Appendix D.
1
The specific nations included in each region are listed in the “Global Metrics by Region” section of this Report. For purposes of this analysis, the
Northwest Territories and Nunavut in Canada shall be considered one jurisdiction.

www.journalofnursingregulation.com 5Volume 10
•
Special Issue
•
January 2020
Global View of Regulatory Atlas Data
Regulation and Governance
Even before Nightingale, religious sisterhoods introduced nursing regulation in the mid-19th century by instituting female matrons in
hospitals and empowering them with authority over training programs, nurses, and female servants.
2
As a regulated profession, nursing
is governed by a set of laws and rules that outline the core tenets of nursing practice, which include (a) profession entry requirements;
(b) how nurses are authorized to practice; (c) what nurses are allowed to do; (d) whether continuing competence must be demonstrated
and with what frequency; (e) which actions warrant discipline and the nature of that discipline; and (f) any other requirements deemed
necessary to protect the public. This section presents an overview of the types of the governing bodies managing nursing regulation
worldwide, their responsibilities and mandates and the composition and qualifications of their members.
Nursing Regulatory Bodies
Regulations and governing of the practice of nursing are managed by regulatory bodies. These may be independent nursing bodies
consisting primarily of nurses, or these may be larger government agencies that also oversee other healthcare professions.
The majority of jurisdictions (97%, n = 312) have a law or set of laws that regulate or govern nurses. Only eight (3%) indicated
that such regulation is not placed in any statute or law.
Nearly all jurisdictions have some form of official regulatory body that oversees nurses.
3
Of the 317 jurisdictions with a nursing
regulatory body (NRB), the majority (66%, n = 208) strictly govern nursing and are referred to as “independent bodies” throughout
the Global Profile (Figure 1). Another 31% (n = 98) of jurisdictions are part of a larger agency. This includes departments such as the
Ministry of Tourism, Public Health, and Sports (Aruba); the Federal Ministry of Labour, Social Affairs, Health and Consumer Protection
(Austria); or the Federal Public Service of Health, Food Chain Safety and Environment (Belgium).
4
The remainder of regulatory bodies
have unique structures that do not fall into either category.
FIGURE 1
Nursing Regulatory Bodies Worldwide (N=317)
Unique Structures (n=11)
Part of a Single Multidisciplinary Body (n=98)
Function Independently (n=208)
31%
3%
66%
2
Early examples include the religious sisterhood at St. John’s House in England, founded in 1848, which assumed responsibility for the nursing ser-
vice of King’s College Hospital in 1855 and Charing Cross Hospital in 1866. See Wildman, S., & Hewison, A. (2009). Rediscovering a history of
nursing management: From Nightingale to the modern matron. International Journal of Nursing Studies, 46, 1650–1661.
3
Three do not: The countries of Georgia, Mongolia, and Togo (though Togo is currently in the process of forming such a body).
4
Other examples of healthcare-related (but not necessarily healthcare-exclusive) multidisciplinary bodies include the Ministry of Health and Social
Security (Cape Verde); the Ministry of Health and the Interior (Faroe Islands); the Ministry of Public Health and Social Assistance (Guatemala); the
Ministry of Health, Labour and Welfare, Nursing Policy Division (Japan); the Department of Health and Social Affairs (Monaco); the Ministry of
Health, Welfare and Sport (Netherlands); and the Ministry of Public Health and Social Welfare (Paraguay).
Part I

6 Journal of Nursing Regulation
NRB Mandates
The majority of NRBs included in this report (95%, n = 301) describe their mandate as the protection of the public (Figure 2), although
many (56%, n = 179) have multiple mandates. Other mandates of regulatory bodies also promote the nursing profession (53%, n = 167)
while roughly a quarter also deal with workforce and labor issues (26%, n = 81).
FIGURE 2
Nursing Regulatory Body Mandates (N=372)
0 20% 40% 60% 80% 100%
Multiple mandates (n=179)
Protection of the public (n=301)
56%
95%
As illustrated in Figure 3, the most common governance responsibility is the power to authorize nurses for practice (94%, n = 298).
NRBs are also responsible for the administration of nursing law and regulation (89%, n = 281). Nearly half (48%, n = 151) also play
some part in the process of creating legislation that applies to nurses. NRBs are also commonly authorized to discipline nurses (85%,
n = 269) and to determine the scope of practice for the nurses in their jurisdiction (78%, n = 247).
FIGURE 3
Governance Powers of Nursing Regulatory Bodies (N=317)
0 20% 40% 60% 80% 100%
Approve Nursing Education in Jursidiction (n=247)
Create Legislation That Applies to Nurses (n=151)
Administrate Nursing Law and Regulation (n=281)
Determine the Scope of Practice (n=247)
Discipline Nurses (n=269)
Authorize Nurses for Practice (n=298)
94%
78%
48%
89%
78%
85%
Composition and Qualifications of NRB
The mean size of nursing regulatory bodies is 17 members, with a median of 13 members. Manipur, India, has the smallest regulatory
body with only two members. Portugal has the largest regulatory body with 153 members.
Of the jurisdictions with an NRB, 184 (58%) specify prerequisites or qualifications an individual must have to serve on that body
(Figure 4). The most common requirement is that each position on the regulatory body must be held by someone with a specific role or
specific expertise. Members of the public who are not part of the nursing profession are commonly required to fill at least one or more
positions on the NRB. More than one third (35%, n = 110) of regulatory bodies have a member of the public serving on the NRB. Sixty-
six jurisdictions (21%) are statutorily required to include at least one government official or public servant, such as a representative from
the ministry of health. Physicians are involved in the NRB in 62 jurisdictions (20%) worldwide. Forty regulatory bodies (13%) include
ex-officio members in their regulatory body proceedings and 35 (11%) specify that a midwife must be included in the regulatory body.

www.journalofnursingregulation.com 7Volume 10
•
Special Issue
•
January 2020
FIGURE 4
Qualifications for Nursing Regulatory Body Members (N=184)
0 5% 10% 15% 20% 25% 30% 35%
Gender Requirements (n=5)
Nursing Professional Organizations Representatives (n=6)
Ministry of Education Representatives (n=6)
Chief Nurse Ofcers (n=9)
Public Health Ministers or Organizations (n=11)
Private Nursing or Home Health
Industry Representatives (n=11)
Member of the Country's Medical Regulatory Body
Who Also Participates in the NRB (n=12)
Lawyers or Other Legal Experts (n=15)
Members of Other Health Professions (n=23)
Nursing Assistants or Technicians (n=26)
Nurse Educators (n=29)
Ex-ofcio Members (n=40)
Physicians (n=62)
Government Ofcial/Public Servant (n=66)
Member of the Public (n=110)
8%
20%
21%
35%
13%
9%
2%
2%
2%
3%
3%
3%
4%
5%
7%
Note. NRB=nursing regulatory body.
Other roles often required on NRBs are nurse educators (9%, n = 29), nursing assistants or technicians (8%, n = 26), members of
other health professions (7%, n = 23), lawyers or other legal experts (5%, n = 15), a member of the country’s medical regulatory body
who also participates in the NRB (4%, n = 12), representatives from the private nursing or home health industry (3%, n = 11), public
health ministers or organizations (3%, n = 11), chief nurse officers (3%, n = 9), representatives from the Ministry of Education (2%,
n = 6), and representatives from nursing professional organizations (2%, n = 6).
Two percent (n = 5) of all jurisdictions included gender requirements for their members. Kenya stipulates that “the Council must
reflect the regional and other diversities of the people of Kenya and not have more than two-thirds of the members be of the same gender.”
French regions, such as Martinique and French Guiana, require their regulatory bodies comprise members of different sexes—in keeping
with France’s laws on gender equality since 1999.
5
In Bihar, India, one of the two registered medical practitioners on the NRB must be
a woman. Two of the three non-officials sitting on the board must also be women. Madhya Pradesh, India, mandates that at least one
male nurse serve among the three members of its Council elected by registered nurses (RNs). In the United States, Iowa mandates that
its regulatory body be party- and gender-balanced.
Apart from specifications that NRB members must hold a certain citizenship or be of a specific nationality (13%, n = 40), live
in a specific area (5%, n = 17), or hold a specific type of nurse license (6%, n = 18), most other requirements concern the character and
expertise of the members. Twenty-eight jurisdictions (9%) require NRB members to have active nursing licenses, and nearly as many
(n = 27) specify a certain number of years in the field as a prerequisite for serving. Twenty-one jurisdictions (7%) specify that members
cannot have legal disputes or cases in progress. Eighteen jurisdictions (6%) require a certain level of education in order to be eligible to
serve, and fifteen require that the members be in good standing or of good moral character. Thirteen jurisdictions (4%) mention political
affiliations of members. In China, for example, nursing council members must “adhere to the outstanding Chinese Communist Party’s
line, principles, policies, and political quality.”
The method used to select members for the regulatory body varies worldwide (Figure 5). In 80 jurisdictions (25%), NRB members
are appointed by a government authority. Fifty-six jurisdictions (18%) elect these officials, while in 39 jurisdictions (12%), officials are
5
See European Parliament, Directorate General for Internal Policies (2011). Electoral Gender Quota Systems and Their Implementation in Europe. https://
www.ndi.org/sites/default/files/Electoral%20Gender%20Quota%20Systems%20and%20Implem_Europe.pdf

8 Journal of Nursing Regulation
nominated by members of the nursing profession, then subject to approval by the government. In many of the remaining jurisdictions,
officials serving on the regulatory body are selected via a combination of these methods. For example, nurse positions on the regulatory
body may be nominated, while the non-nurse positions may be appointed.
FIGURE 5
Nursing Regulatory Bodies Selection Methods
Appointed by a Government Authority (n=80)
Elected (n=56)
Nominated by Members of the Nursing Profession (n=39)
Other, or Some Combination of the Above (n=142)
45%
18%
12%
25%
Licensure and Registration Requirements to Practice
Data on nursing licensure and the various requirements to practice and legislation in each jurisdiction, including how to obtain autho-
rization to practice, are presented in this section. Additionally, data on mobility of the nursing workforce and compacts and mutual
agreements are discussed.
Authorization to Practice
As reflected in Figure 6, half (50%, n = 160) of the 320 jurisdictions authorize nurses to practice via registration, while 31% (n = 100)
license nurses to authorize them to practice. In 6 jurisdictions, no registration or licensure is necessary (Argentina, Armenia, Cape Verde
[Cabo Verde], Georgia, Mauritius, and Togo); general (or registered) nurses are considered authorized to practice when they complete
their education. Seven jurisdictions (Burkina Faso, Gabon, Mauritania, Mauritius, Niger, Papua New Guinea, and Uzbekistan) con
-
sider midwives authorized to practice when they complete their education. Quebec, Canada, considers nurse practitioners authorized to
practice when they complete their education.
The 16 Middle Eastern jurisdictions are split as to how they grant practice authorization to the nursing profession.
6
Four coun-
tries grant authority to practice via registration. The remaining jurisdictions are divided evenly between NRBs that grant authority
to practice by both license and registration and NRBs that allow professional practice by certification or after successful completion of
training and education.
6
For the purposes of this report, Middle Eastern jurisdictions consisted of Armenia, Azerbaijan, Bahrain, Georgia, Iran, Iraq, Israel, Jordan, Kuwait,
Lebanon, Oman, Palestine, Saudi Arabia, Syrian Arab Republic, United Arab Emirates, and Yemen. As Cyprus is a member of the European Union,
analysis of Eastern Europe included Cyprus for jurisdictional convenience.

www.journalofnursingregulation.com 9Volume 10
•
Special Issue
•
January 2020
FIGURE 6
Jurisdictional Methods of Authorization to Practice (N=320)
0
20 40 60 80 100 120 140 160 180
Upon Completion of Education
Licensure
Registration
160
10
100
A common practice throughout the world is to compile a nurse register, or roll, which is a list or database of every nurse currently
authorized in a jurisdiction. Many NRBs (73%, n = 233) make this register available to the public. Providing the register publicly
may entail posting it online, publishing it in an official publication of the jurisdiction (eg, a national gazette), or providing a physical
copy at the NRB office.
Most of Western and Central Europe maintain an online, public database or registry of nursing professionals. This includes Austria,
Belgium, the Czech Republic, France, Germany, Hungary, Ireland, Italy, Luxembourg, the Netherlands, Slovenia, Spain, Switzerland,
and the United Kingdom.
Currently, Andorra, Liechtenstein, Malta, and Slovakia only provide the public with access to a physical database, such as a news
-
paper, stored at the Ministry of Health’s headquarters. Data are not available as to whether a physical database is accessible in Monaco
or San Marino. Poland and Portugal restrict all registry access and related disciplinary record information.
In addition to verifying a nursing professional’s credentials, notifications of past or current disciplinary actions are often also pub
-
licly accessible as part of a nursing registry. In terms of discipline, the following actions are commonly taken in Western and Central
Europe: reprimand, suspension, fine/civil penalty, denial or withdrawal of license, surrender of license, removal or denial of name from
register, revocation, practice limitation, probation, censure, and warnings.
Fitness to Practice
Fitness to practice comprises the requisite skills, knowledge, competence, health, and character to practice within the nursing profes-
sion. This may include evidence of moral character such as criminal background checks and references. Three quarters of all jurisdictions
(n = 240) require nurses to provide evidence of good moral character to become authorized, or maintain their authorization, to practice.
This evidence is provided in a variety of ways. In Brazil, for example, evidence is defined as “attestations of moral suitability,” whereas
in Alberta and British Columbia, Canada; Bermuda; Cyprus; Denmark; Germany; Unites States; and other jurisdictions it consists of
a criminal record (or background) check. In Andhra Pradesh, India, three individuals must attest to the nurse’s good moral character:
one attestation must be from a person with good social standing and not related, another from an employer, and the third must be from
a school superintendent or medical practitioner. Azerbaijan requires personnel records and a statement from employers to satisfy the
moral character requirement.
Apart from moral character, the most common additional fitness to practice requirement employed by NRBs is proof of proficiency
in a particular language. Forty-five percent of jurisdictions worldwide (n = 143) specify that such a requirement is in place.
National Examination Requirements
Only 22 (6%) NRBs do not possess the authority to require nursing applicants to take a qualifying examination before becoming au-
thorized to practice; however, not all NRBs with the authority to do so have opted to require such an examination. About two thirds of
jurisdictions (67%, n = 214) require a nurse to pass a qualifying examination before he or she is permitted to practice.
North American and the Caribbean
With the exception of Quebec, which has a province-specific set of licensure examinations, the United States and Canada require all
candidates for nursing licensure or registration to pass the National Council Licensure Examination-RN (NCLEX-RN). For licensed
practical and licensed vocational nurses (LPN/LVN), the United States requires the NCLEX-PN; Canadian practical nurses take the
Canadian Practical Nurse Registration Examination (CPRNE). A licensing or qualifying examination is required for nearly every nurse
type in the United States and its territories. The powers granted to all regulatory bodies throughout Canada include the authority to
require a national examination to practice.

10 Journal of Nursing Regulation
In addition to educational requirements, graduation examinations are required for master’s-level and doctoral-level nurses in
Mexico. Licensed nurses are required to pass the Centro Nacional para la Evaluación de la Educación Superior (Ceneval) examination to
practice, but no examinations are required for the remaining nursing types.
In Central America, Costa Rica, El Salvador, and Nicaragua require a national examination after education is completed. Honduras
does not require a national examination for their nurses. There are no data publicly available for Guatemala.
The Caribbean Community (CARICOM) requires a national examination to practice nursing. Nurses trained in Bermuda must
sit for the NCLEX in New York State in the United States.
7
South America
Qualifying examinations are widely mandated throughout South America. They are required for all nurse types in Bolivia, as well as for
nurses, midwives, and nursing assistants in Chile. Nurses and midwives in Ecuador and Peru must pass a qualifying examination. It is
unknown if a national qualifying examination is required in almost all Brazilian states.
Europe
Almost all NRBs in the Nordic region have the authority to require a national examination to practice nursing. Denmark is the lone
exception and shares such decision-making power with the Ministry of Education and the National Board of Health.
8
Of 22 Western and Central European countries, most require a national examination to practice, except for Belgium, Ireland,
Poland, Portugal, Switzerland, and the United Kingdom that do not. A national examination is required to practice nursing in Eastern
Europe, except for Albania, Croatia, Estonia, and Romania.
Africa
Nearly all African jurisdictions require nurses to complete an examination prior to beginning their practice. Cape Verde is the only
African nation (for which information is publicly available) in which no nurse roles have an examination requirement for practice.
Botswana, Gambia, and Mauritius each require national examinations for some nursing roles, but not others.
Middle East
Iran requires passage of an examination after the necessary education to become a general nurse, but no such examination is required
for practical nurses or nurse anesthetists. Saudi Arabia requires passage of the Saudi Nursing Licensure Examination to become a nurse,
a nurse specialist, or a nurse assistant.
Asia
Nearly all East Asian nations require a national examination for all nurse roles. Hong Kong requires only applicants trained outside of
Hong Kong to take its jurisdictional examination prior to practicing.
Except for Uzbekistan, every jurisdiction in Central Asia requires nursing candidates to pass a qualifying examination after successful
completion of a nursing program.
9
In India, the majority of state jurisdictions require a qualifying examination for most nurse types.
10
NRBs in the Southeast Asia region have the authority to require a national examination to practice, except for Cambodia.
11
Although
not every Southeast Asian country requires a national examination, the majority do, including Brunei, Laos, Malaysia, Myanmar, the
Philippines, and Thailand. It is not clear what position Indonesia takes concerning this requirement.
Australia and Oceania
Nearly all nations in Oceania require a qualifying examination for all nurse roles. Australia does not require an examination of any of
its nurse roles; New Zealand does not have an examination requirement for its nurse prescriber roles.
Jurisdictions Not Requiring Examination
Thirty-three of all reporting jurisdictions either do not require an examination for general (or registered) nurses after completion of edu-
cation, or no evidence existed of any relevant legislation in this regard. These jurisdictions are as follows: Argentina, Australia, Belgium,
7
The Bermuda College Nursing Education Program has an agreement with the New York State Board of Nursing.
8
The Nordic region encompasses Denmark, Faroe Islands, Finland, Greenland, Iceland, Norway, and Sweden. Of those countries, Denmark, Finland,
and Sweden are members of the European Union (EU). Additionally, all are Nordic Passport Union members.
9
No data could be found on whether Uzbekistan requires such an examination.
10
In India, there is typically no qualifying examination for post-basic and specialty nurse type designations. However, university examinations or addi-
tional qualification in some respect of the training specialty is required.
11
It is not clear whether the Indonesian Ministry of Health maintains this authority as far as nursing powers are concerned.

www.journalofnursingregulation.com 11Volume 10
•
Special Issue
•
January 2020
Cambodia, Cape Verde, Croatia, Gambia, Honduras, Hong Kong, Iceland, 14 jurisdictions in India (the Andaman and Nicobar Islands,
Andhra Pradesh, Bihar, Chandigarh, Chhattisgarh, Delhi, Jammu and Kashmir, Odisha, Puducherry, Punjab, Tamil Nadu, Telangana,
Uttar Pradesh, and Uttarakhand), Ireland, Jordan, Lithuania, Mauritius, Poland, Qatar, Singapore, United Kingdom, and Vietnam.
Nurse Mobility: Compacts and Mutual Agreements
To facilitate an increasingly mobile and globalized workforce, many jurisdictions have entered into compacts or mutual agreements
with other jurisdictions. These agreements make it easier for a nurse authorized to practice in one jurisdiction to become authorized
in another. In some cases, these agreements are accomplished through the alignment of education and licensure regulations. In other
cases, two or more jurisdictions agree to mutually recognize any nurse that is licensed in one of the member jurisdictions. Of the 320
jurisdictions, 45% (n = 147) were part of a mutual agreement or compact (Figure 7).
12
North American and the Caribbean
In the United States, the Nurse Licensure Compact (NLC) is a mutual recognition agreement created to increase the mobility of registered
and practical nurses’ patient access while maintaining the protection of the public at the state level. At the time of this publication, 34
jurisdictions participate in the NLC.
13
By removing the need to obtain additional state licenses, the NLC provides ease of access across
state borders, which is vital in the event of an emergency or disaster. The NLC allows nurses, who meet designated requirements, to
obtain a license in their home state and practice in other states without obtaining an additional license. It eliminates the financial burden
of multiple licenses and facilitates telehealth nursing, and mobility during disasters along with many other advantages.
FIGURE 7
Compacts and Agreements Among Jurisdictions
Engaged in Mutual Agreements or Compacts (n=145)
No Mutual Agreements or Compacts (n=175)
45%
55%
There are 14 members of the Canadian Free Trade Agreement (CFTA), which enables any worker certified for an occupation by
one of its members, including nursing professionals, to be recognized as qualified for that occupation by all other members.
14
Europe
Specifically related to the nursing profession and mobility, EU Directive 2005/36/EC came into effect in October 2007 and provided
for the acceptance and recognition of professional qualifications across member states. This allows for mobility of nursing professionals
throughout much of Europe.
12
Four African jurisdictions responded that they had such an agreement but are not counted in these jurisdictions because they referenced compacts
that do not directly affect the practice of nursing across borders.
13
Participants include the states of Alabama, Arizona, Arkansas, Colorado, Delaware, Florida, Georgia, Idaho, Indiana, Iowa, Kansas, Kentucky, Loui-
siana, Maine, Maryland, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Jersey, New Mexico, North Carolina, North Dakota,
Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, West Virginia, Wisconsin, and Wyoming. Alabama’s NLC membership
was implemented January 1, 2020. Indiana and New Jersey have enacted the NLC and are awaiting implementation.
14
These include Canada (federal), Ontario, Quebec, Nova Scotia, New Brunswick, Manitoba, British Columbia, Prince Edward Island, Saskatchewan,
Alberta, Newfoundland and Labrador, The Northwest Territories, Yukon, and Nunavut.

12 Journal of Nursing Regulation
Asia
Currently there are 10 member countries that belong to the Association of Southeast Asian Nations (ASEAN), which provides for the
Mutual Recognition Arrangement of nursing services.
15
The Mutual Recognition Arrangement allows for the mobility of nursing pro-
fessionals within Southeast Asia; the exchange of nursing expertise suited to the specific needs of ASEAN member countries; adoption
of best practices; and provision of training opportunities throughout the region.
Australia and Oceania
Today, enrolled nurses, RNs, and nurse practitioners are mutually recognized throughout Australia and New Zealand through the
Trans-Tasman Mutual Recognition Act.
Nurse Types and Titles
Throughout the world, there are at least 220 unique nurse titles. Overall, most nurse types throughout the world fit into one of four
categories: nurse, specialized nurse, midwife, or nurse assistant.
A diverse array of classifications for specialized nurses occupies a large proportion of the remaining unique nurse titles. For ex
-
ample, in addition to a general nurse, Saudi Arabia recognizes General Specialists 1 and 2 and First Specialists 1 and 2, which are all
types of nurse specialists. These nurse specialists are categorized by education, training, and competence. Brunei recognizes children’s
nurses, mental health nurses, and infectious disease nurses in terms of specialized nursing. In addition to a RN, licensed practical nurse
(LPN), and nurse anesthetist, Liberia has an ophthalmic nurse. Malaysia recognizes public health nurses and community nurses, and
Thailand also recognizes nurse anesthetists.
In the United States, there are three main nurse types: RNs, LPNs, and advanced practice registered nurses (APRNs). There are
four different types of advanced practice nurses that includes certified nurse practitioners, certified nurse midwife, clinical nurse special
-
ist, and certified registered nurse anesthetists.
In Lebanon, there are RNs and technique superior RNs—a form of specialty nurse. A Lithuanian general nurse is known as a
nurse general practitioner, or general practitioner, and a nurse with a master’s in nursing is known as a nurse general practitioner and
professional.
Several jurisdictions around the world incorporate educational levels into nurse titles (Table 1). Mexico incorporates educational
levels into its nurse titles, which often results in designations such as master’s nurse, postgraduate nurse, and doctoral nurse. Macao
has a Grade I Nurse, who must pass an entrance exam, and a nurse graduate, who is a Grade I Nurse with 3 to 4 years of experience. In
Liberia, graduate nurses are graduates of a nursing program who are awaiting nursing licensure and may practice under the supervision
of an RN or an LPN.
16
15
These include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, the Philippines, Singapore, Thailand, and Vietnam.
16
“Graduate nurse” is a capacious category that can refer to a range of nursing levels, depending on the jurisdiction.
www.journalofnursingregulation.com 13Volume 10
•
Special Issue
•
January 2020
TABLE 1
Jurisdictions That Incorporate Educational Levels Into Recognized Nurse Types
Region Jurisdiction Recognized Nurse Types
Africa Ethiopia Bachelor of Nursing
Master’s Nurse
Gambia Bachelor of Nursing
Master’s in Nursing
Madagascar Master’s in Nursing
The
Caribbean
Cuba Bachelor of Science in
Nursing
Doctorate in Nursing
Central
America
El Salvador Bachelor of Nursing
Guatemala Bachelor of Nursing
Master’s in Nursing
PhD nurse
Honduras Master’s Nurse
Central Asia
and India
Bhutan Bachelor of Nursing
Master’s in Nursing
India—Andhra
Pradesh
Bachelor of Nursing
Master’s Nurse
India—Arunachal
Pradesh
Bachelor of Science in
Nursing
India India—Bihar Bachelor of Nursing
Master’s Nurse
India—Chandigarh Bachelor of Nursing
Master’s in Nursing
India—Chhattisgarh Bachelor of Nursing
Master’s in Nursing
India—Haryana Bachelor of Nursing
Master’s in Nursing
India—Jammu and
Kashmir
Bachelor of Nursing
Master’s in Nursing
India India—Kerala Master’s in Nursing
Ph.D. Nursing
M. Phil Nursing
India—Madhya
Pradesh
Bachelor of Nursing
Master’s in Nursing
PhD nurse
India—Manipur Bachelor of Nursing
India—Odisha Bachelor of Nursing
Master’s in Nursing
Doctoral Nurse
Region Jurisdiction Recognized Nurse Types
Central Asia
and India
(continued)
India—Punjab Bachelor of Nursing
Master’s in Nursing
India—Rajasthan Master’s in Nursing
India—Sikkim Master’s in Nursing
India—Telangana Bachelor of Nursing
Master’s Nurse
India—Uttar
Pradesh
Bachelor of Nursing
Master’s in Nursing
India—Uttarakhand Bachelor of Nursing
Master’s in Nursing
India—West Bengal Master’s in Nursing
China and
East Asia
China Associate Nurse
Bachelor of Nursing
Master’s Nurse
Doctoral Nurse
Mongolia Bachelor Degree Nurse
Master’s Nurse
PhD nurse
Eastern
Europe
Croatia Bachelor of Nursing
Mexico Mexico Master’s Nurse
Doctoral Nurse
Middle East Saudi Arabia PhD Nurse/Advisory Nurse
South
America
Chile Master’s in Nursing
Doctoral Nurse
Colombia Undergraduate Nurse
Master’s in Nursing
Doctorate in Nursing
Postdoctoral Nurse
Cambodia Bachelor of Science in
Nursing
Associate Degree Nurse
Southeast
Asia
Laos Associate Nurse (also
known as Registered
Nurse / High-level nurse)
Bachelor Level Nurse (also
known as Graduate Nurse)
Western and
Central
Europe
Hungary Bachelor of Nursing
Master’s in Nursing
Poland Bachelor of Nursing
Master’s Nurse
Other Titles, Roles, and Responsibilities
Some nurse titles are evocative of community culture and history. For example, some African jurisdictions, such as Cameroon and the
Republic of Congo, designate a “qualified wise woman” or a “qualified sage-femme” as a midwife nurse type. Thousands of African wise

14 Journal of Nursing Regulation
women were enslaved and transported to the Western Hemisphere from the 16th century onward, where many continued to practice or
passed down their knowledge, and eventually became known in the American South as “granny” or “grand” midwives.
17
The “wise woman” category dates to antiquity. It was not always synonymous with midwifery in Europe but was associated with
women as public healers and problem-solvers. The first known English midwife’s license dates from 1588, but the licensure process came
about long after the role came into existence. Midwives also appear in the fifth-century BC writings of Chinese philosopher Lao Tzu.
18
A lady health visitor (LHV), as noted by Upvall et al (2002), can provide a range of healthcare services depending on the context,
including “basic nursing care, maternal child health services, and training of community workers.” In some cases, as in Pakistan, “LHVs
aligned their practice with medicine yet were originally registered with the Pakistan Nursing Council and had 1 year of midwifery
training [Pakistan currently reports that LHV training takes 2 years]. LHVs also differentiated their practice from nursing by clearly
demarcating the role of RNs to the hospital, whereas they as LHVs served the community.”
19
In Pakistan, the LHV program is for
females aged between 15 and 30 years only.
20
An LHV is also recognized in the Indian states of Manipur, Sikkim, and West Bengal.
A community LHV is recognized in Myanmar. Twelve states and three union territories in India recognize a health visitor (or licensed
health visitor), as do Cyprus and Denmark.
21
The South Pacific archipelago of Vanuatu has a village health worker who is chosen by the
community and whose training program takes 11 weeks to complete. In the historical record, references to LHVs date back to 1909 in
Wales, 1911 in Canada, and 1951 in Pakistan
Some Indian states, such as Punjab, used to account for a very traditional form of birthing attendant called a dai. A dai provides
birthing and midwifery care in rural parts of India and has not passed any form of official certification. References to dais are found in
older nursing regulations. More recent nursing acts and regulations recognize registered midwives and nurse midwives.
Midwives
In the United States, there are four main types of midwives: CNMs, certified midwives (CMs), certified professional midwives (CPMs),
and other (or lay) midwives. The vast majority are CNMs, who are RNs with graduate education and clinical training in midwifery.
CMs possess a bachelor’s degree in an area other than nursing but also have graduate midwifery education. Both CNMs and CMs must
pass the national certification examination of the American Midwifery Certification Board. Both CNMs and CMs are able to provide
care across a woman’s lifespan, not just during maternity and labor, have the authority to prescribe medications and treatments, and
work in a variety of healthcare settings, such as hospitals, birth centers, private practice, and even homes.
22,23
CPMs are educated by means of one of two pathways: (1) through apprenticeship training alone or (2) through an accredited
formal education program. All CPM candidates must pass the national certification examination administered by the North American
Registry of Midwives. CPMs are much more limited in the services they provide—they provide only pregnancy, birth, and postpartum
care for women outside of the hospital, usually in birth centers and homes, and they cannot prescribe medication or treatments.
24
By
comparison, lay midwives are not formally trained, educated, or certified. They are often unlicensed and usually work in the home setting.
25
As of 2018, CNMs are regulated by their state board in 79% of U.S. jurisdictions (n = 45 of 56 total). The state board of medi
-
cine or medical examiners regulates nurse midwives in 5 states: Alabama, North Carolina, New Jersey, Pennsylvania, and Virginia. In
Nebraska, the Advanced Practice Nursing Board regulates CNMs, while in 4 states—Connecticut, Michigan, New Mexico, and Rhode
Island—the department or board of health oversees nurse midwife regulation. In Utah and New York, a nursing board under a state
agency regulates CNMs.
17
The term “granny” carries its own historical controversy. As Goode (2014) explains, “there is often a historical assumption that granny midwives
relied solely on ‘divine intervention’ because of ‘the call’ to be a midwife.” Instead, Goode employs the term “grand midwives.” See Goode, K.
(2014). Birthing, Blackness, and the Body: Black Midwives and Experiential Continuities of Institutional Racism (pp. 49–50) [Doctoral dissertation]. The
City University of New York. https://academicworks.cuny.edu/gc_etds/423
18
On Lao Tzu’s writings about midwives, see Chamberlain et al., 2016.
19
Upvall, M. J., Sochael, S., & Gonsalves, A. (2002). Behind the mud walls: The role and practice of lady health visitors in Pakistan. Health Care
Women Int., 23(5), 432–441.
20
Pakistan applies the same females-only rule to its programs for licensed practical nurses and family welfare workers.
21
Those Indian states are Arunachal Pradesh, Chhattisgarh, Gujarat, Himachal Pradesh, Karnataka, Kerala, Madhya Pradesh, Meghalaya, Odisha,
Punjab, Rajasthan, and Tripura. The 3 Indian union territories are Chandigarh, Dadra and Nagar Haveli, and Daman and Diu.
22
Fotsch, R. (2017, July). Regulating certified professional midwives in state legislatures. Journal of Nursing Regulation, 8(2), 47–49; American College
of Nurse-Midwives. (2016, November 23). What is a midwife? http:// ourmomentoftruth.com/your-health/what-is-a-midwife/
23
Fotsch, R. (2017, July); American College of Nurse-Midwives. (2016, November 23).
24
Fotsch, R. (2017, July); American College of Nurse-Midwives. (2016, November 23).
25
Fotsch, R. (2017, July); American College of Nurse-Midwives. (2016, November 23).

www.journalofnursingregulation.com 15Volume 10
•
Special Issue
•
January 2020
Eleven of 16 Middle Eastern nations recognize some type of midwife, and six of them require a qualifying examination.
26
Azerbaijan
identifies three separate midwifery categories: nurse midwife, midwife, and auxiliary midwife. Most Middle Eastern midwifery programs
are approximately 3 years in duration and require completion of grade 10 or all of secondary school education.
As noted previously, a few African jurisdictions designate a unique title to what is commonly referred to as a midwife. The
Cameroon Ministry of Public Health, in particular, designates a qualified wise woman or a qualified sage-femme as a midwife. Similarly,
the Republic of Congo designates a wise woman as a midwife nurse type. Thirty-four out of 54 African nations recognize at least one
type of midwife, whose training program requires an average of 2.75 years and completion of secondary school education. In Gabon,
midwives are considered authorized upon completion of their nursing education and training in midwifery.
In Vietnam, midwives—like nurses—are distinguished by their level of education: elementary midwives have 1 year of train
-
ing, secondary midwives have 2 years, college midwives have 3 years, a midwife has completed 4 years, and an advanced midwife has
completed an additional 2 years.
Afghanistan recognizes at least 3 types of midwives: an assistant midwife (who must pass the Afghan National Testing and
Certification Midwifery Examination), an auxiliary nurse midwife (requiring 6 months of training), and a community midwife (requir
-
ing 2 years of training).
Education
The approval and accreditation of nursing programs varies by jurisdiction. Figure 8 presents the general nursing (RN) programs world-
wide and the average number of years it takes to matriculate.
FIGURE 8
Average Duration of General Nursing (RN) Programs
0 1 2 3 4 5
United States (n=41)
Mexico (n=1)
Australia and Oceania (n=12)
Africa (n=21)
Central Asia and India (n=6)
China and East Asia (n=6)
Western/Central Europe (General Nurse), (n=20)
Southeast Asia (n=9)
Middle East (n=8)
Nordic Countries (General Nurse), (n=5)
Eastern Europe (n=10)
Canada (n=10)
Non-CARICOM Caribbean Nations (n=3)
CARICOM (n=3)
CARICOM (n=13)
South America (n=3)
Central America (n=3)
3.4
3.7
3.7
3.7
4.2
4.3
3.6
3.5
2.9
Average Duration of General Nursing (RN) Programs (in years)
3
3.1
3.2
3.3
3.3
3.3
3.4
3.4
Note. CARICOM=Caribbean community; RN=registered nurse.
Nursing Program Approval
Seventy percent (n = 223) of the 317 NRBs worldwide are responsible for approving nursing education within their jurisdictions. The
remainder may share this responsibility, or it may be handled by the jurisdiction’s Ministry of Education.
26
Middle Eastern nations that recognize a midwife, registered midwife, or nurse midwife are Azerbaijan, Bahrain, Iraq, Israel, Jordan, Kuwait, Oman,
Palestine, Syrian Arab Republic, United Arab Emirates, and Yemen. Those requiring a qualifying examination for midwives are Azerbaijan, Bah-
rain, Iraq, Israel, Palestine, and United Arab Emirates.

16 Journal of Nursing Regulation
North American and the Caribbean
The powers granted to all regulatory bodies throughout Canada, the United States, and U.S. territories include the authority to approve
nursing programs, with three exceptions in the United States. In New York, the Professional Education Program Review Office coordi
-
nates all registration for educational programs in the state. The power to approve nurse training and education programs in Mississippi
is reserved for the Institutions of Higher Learning, the regulatory body for higher education in the state of Mississippi; and in Utah,
approval of programs is delegated to a nationally recognized accrediting body.
Authorization of nursing programs is done by each Ministry of Health in CARICOM member states. Among CARICOM associate
members, the British Virgin Islands and Anguilla hold the power to approve nurse education and training programs.
Nursing education programs in Mexico are approved by the Secretary of Health and Secretary of Public Education. Almost all
Central American regulatory bodies have the authority to approve nursing schools or programs.
South America
Of all the governing regulatory bodies in the South American jurisdictions, the College of Nurses of Peru and the College of Nursing
Professionals of Venezuela hold exclusive authority to approve nursing education programs. Education programs for nursing professionals
in other jurisdictions are either approved by a separate governing agency, such as the Ministry of Education, or the NRB in cooperation
with a separate agency. For example, the Ministry of Education approves nurse education programs in Brazil. In Bolivia, the Ministry of
Health works in cooperation with the Bolivia National Council of Higher Education and the Bolivia Ministry of Education to approve
programs. Similarly, each respective Ministry of Education works in conjunction with the nursing regulatory body in Chile, Ecuador,
Paraguay, and Uruguay. In Colombia, a separate College of Association of Nursing Faculty approves programs.
Europe
The Nordic NRBs with smaller populations, such as Iceland, Faroe Islands, and Greenland, approve nursing programs. However, in
more populous countries, such as Norway, Sweden, Denmark, and Finland, the authority to approve nursing programs or schools is
reserved for the Ministry of Education.
In Western and Central Europe, NRBs in Andorra, Ireland, Italy, Portugal, Spain, and the United Kingdom approve nursing
schools or programs. In France, Germany, Malta, and Slovakia, it is the responsibility of the Ministry of Education and the Ministry of
Health. Only Belgium and the Netherlands do not designate their respective Ministry of Health agencies to approve nursing education
programs, while the other Western and Central European countries do. In Belgium and The Netherlands, the Ministry of Education is
charged with this responsibility. Some countries retain the authority to approve nursing education programs but also work in conjunc
-
tion with the Ministry of Education in the process, such as in Slovenia and Monaco.
In Eastern Europe, the NRB is responsible for approving nursing education programs in the majority (67%, n = 12 of 18) of
jurisdictions.
Africa
In Africa, the authority to approve nursing schools or programs is commonly vested with nursing regulatory bodies, as 33 such bod-
ies possess sole authority over nursing education. In Rwanda and South Africa, the approval of programs is shared jointly with each
country’s respective higher education authority. In five countries, the responsibility for approving programs is held by other ministries
or agencies. Namely, in Kenya and Togo, the Ministry of Health is responsible; in Ethiopia and the Republic of Congo, the Ministry of
Higher Education is responsible; and in Egypt, the General Directorate of Technical Education for Health approves nursing programs.
Data were unavailable as to how the process is handled in the Seychelles.
Asia
In East Asia, Hong Kong, Japan, and South Korea maintain the authority to approve nursing schools or programs. China, Mongolia,
and Taiwan all reserve such authority to their Ministry of Education organizations.
The nursing profession in Central Asia is primarily governed by larger government agencies, which hold the power to approve
nurse education programs with two exceptions. In Kazakhstan, it is the Ministry of Education along with local regional governments
that authorize nurse education programs. In Sri Lanka, the nursing council division of the Medical Council may advise the government
on matters relating to the education of nursing professionals but does not necessarily have exclusive authority.
Some Southeast Asian regulatory bodies maintain the sole authority to approve nursing schools or programs, including Brunei,
Myanmar, Singapore, and Thailand. Others, including Laos, Malaysia, and the Philippines, share such authority with their respective
Ministries of Education, Qualification Agencies, or Higher Education Commissions. In Cambodia and Vietnam, this authority is reserved

www.journalofnursingregulation.com 17Volume 10
•
Special Issue
•
January 2020
by other branches of the government: the Ministry of Health in Cambodia and the Ministry of Education in Vietnam. Information is
not available as to whether the Indonesian Ministry of Health maintains the authority to approve nursing schools or programs.
Australia and Oceania
Oceania and Australia regulatory bodies are authorized to approve nursing programs.
Continuing Competence
Worldwide, 72% (n = 230) of jurisdictions report that they require nurses to undergo some form of continuing education to remain
authorized to practice. Continuing education may be called continuing competence, continuing professional development, or continu
-
ing fitness to practice.
Practice
Nurses throughout the world have numerous responsibilities and it is beyond the extent of this report to detail all the nursing activities
that are performed throughout the world. We did, however, explore which nurses have expanded responsibilities that encompass three
areas: diagnosis, prescribing, and referrals to another practitioner.
Although researchers in many jurisdictions were unable to gather these data, it was possible to determine that at least 52%
(n = 167) of jurisdictions around the world allow nurses to prescribe medications or other types of treatment to some degree. In 37%
(n = 117) of these jurisdictions, there is at least one nursing role with unrestricted prescribing authority.
Similarly, 51% (n = 165) of jurisdictions allow diagnoses to be made by at least one type of nurse, although in many cases, these
jurisdictions place restrictions on the type of diagnoses the authorized nurse may provide.
Worldwide, 21% (n = 67) of jurisdictions permit RNs to diagnose, though often with limitations (Table 2). A “nursing diagnosis,”
which is an evidence-based clinical judgment that allows a nurse to develop a care plan and select nursing interventions, is codified in
at least 5% (n = 17) of jurisdictions.
27
TABLE 2
Jurisdictions That Allow Registered Nurses to Diagnose
27
In addition to some U.S. jurisdictions, including Guam and the Northern Mariana Islands, these include Brazil (for nurses and advanced or special-
ized nurses); Lesotho, and Madagascar (for registered nurses).
Nation (Sub-jurisdiction)
Albania
Australia
Belgium
Belize
Botswana
Brazil (Alagoas, Amapa, Amazonas, Bahia, Ceara, Distrito Feder
-
al, Espirito Santo, Goias, Maranhão, Mato Grosso, Mato Grosso
do Suul, Pará, Paraiba, Paraná, Pernambuco, Piauí, Rio de Janei
-
ro, Rio Grande de Norte, Rio Grande do Sul, Rondônia, Roraima,
Santa Catarina, Sao Paulo, Sergipe, Tocantins)
Cambodia
Canada (British Columbia, Manitoba, Quebec, Saskatchewan)
Croatia
a
Dominica
El Salvador
Estonia
a
Greece
a
Guam
Haiti
Nation (Sub-jurisdiction)
Honduras
Kazakhstan
Lesotho
Liechtenstein
Madagascar
Marshall Islands
Monaco
Mongolia
Northern Mariana Islands
Peru
Poland
b
Portugal
Rwanda
South Africa
Switzerland
Togo
United Kingdom
Vietnam
Zimbabwe
a
Limited to nursing diagnosis.
b
“To a limited extent.”

18 Journal of Nursing Regulation
Discipline
Almost two-thirds of jurisdictions keep disciplinary records of actions taken against nurses (Figure 9). The NRBs in nine nations do
not maintain records of disciplinary actions taken against nurses. These include Armenia, Cambodia, Chile, China, Georgia, Greece,
Lithuania, Mongolia, and Russia.
Of the NRBs worldwide that keep records of disciplinary action taken against a nurse:
⦁
70% store disciplinary information in the same database that holds the nurse register
⦁
69% make their disciplinary records available to the public
⦁
58% of disciplinary record-keeping jurisdictions retain their disciplinary records indefinitely (Figure 9)
⦁
11% keep records for a defined number of years, ranging from 5 to 75 years (Figure 9).
28
Of all NRBs in this report, including those that do not keep disciplinary records, 43% allow members of the public to access the
disciplinary records of nurses practicing in their jurisdiction.
FIGURE 9
Disciplinary Record Retention Policies for 200 Worlwide Jurisdictions
Retains Records Indenitely (58%)
More Complex Standards for Record Retention (31%)
Keeps Records 5–75 Years (11%)
31%
11 %
58%
28
Many jurisdictions referred to records retention statutes or stated that the length of time the record was retained differed depending on the nature of
the offense. One jurisdiction retained the record for as long as the sanction was in place, while others destroyed such records at such time as the nurse
was no longer authorized to practice or upon the nurse’s death.

www.journalofnursingregulation.com 19Volume 10
•
Special Issue
•
January 2020
Regional View of the
GlobalRegulatoryAtlas Data
The Global Regulatory Atlas data presented in Part II provide a detailed regional view of nursing regulation, education, and practice.
Tables outlining the nursing education program requirements are provided in Appendix C.
Africa
A
frica consists of 54 recognized countries (the sovereign statuses of Somaliland and Western Sahara are currently disputed).
Due to a lack of digitally accessible and verifiable data about nursing regulation, Algeria, Angola, Chad, Equatorial Guinea,
Guinea-Bissau, Sao Tome and Principe, Senegal, Sierra Leone, Somalia, South Sudan, and Sudan are not included in this report.
Regulation and Governance
An independent body—most commonly a nursing council—serves as the nursing regulatory body and governs the nursing profession
in a majority of African jurisdictions. This body is generally a Nursing and Midwifery Council, National Board of Nurses, or National
Order of Nurses. An independent body governs and regulates the nursing profession in Botswana, Burundi, the Democratic Republic of
Congo (or simply Congo), Gambia, Ghana, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mauritius, Mozambique, Namibia, Nigeria,
Rwanda, the Seychelles, South Africa, Eswatini (formerly known as Swaziland), Tanzania, Uganda, Zambia, and Zimbabwe.
In some jurisdictions, the nursing profession is overseen by a regulatory body that supervises other professions as well. In all these
cases, nursing regulation is part of the Ministry of Health or a subdivision thereof. The jurisdictions of Benin, Burkina Faso, Cameroon,
Cape Verde, Côte d’Ivoire, Djibouti, Egypt, Eritrea, Ethiopia, Gabon, Guinea, Libya, Mali, Mauritania, Morocco, Niger, and Tunisia
have this type of structure. Most ministries or governing bodies hold the power to license/register nurses, administer nursing laws and
regulations, discipline nurses, make decisions about the nursing scope of practice, and regulate for purposes of public protection and the
promotion of the nursing profession. These bodies retain the power to create nursing legislation. Except for the Egyptian Ministry of
Health and Population and the Ethiopian Health Professions Council, many larger agency bodies hold the authority to approve nursing
education institutions and programs. Sometimes, each Ministry of Health works in cooperation with a Ministry of Higher Education or
another government department in this approval process. Such is the case with Cameroon, Cape Verde, Congo, Côte d’Ivoire, Guinea,
Libya, and Tunisia.
Regulatory bodies in eight countries (Cameroon, Cape Verde, Eritrea, Ghana, Guinea, Lesotho, Mozambique, and Tunisia) are also
responsible for education and training matters. Ghana and Madagascar specifically mention disciplinary matters among their respon
-
sibilities. Eritrea’s regulatory body also promotes and finances healthcare in addition to matters related to nursing. Finally, in Ghana,
facility inspection is also part of the regulatory body’s role.
The regulatory bodies in Burundi and Liberia possess authority regarding nurse education and training, and continuing competence
or curriculum matters. The governing bodies of nursing in Botswana, Malawi, Mauritius, Mozambique, Rwanda, South Africa, Eswatini,
and Tanzania retain the power to create nursing legislation. The governing bodies in Congo, Madagascar, Mozambique, Nigeria, the
Seychelles, Uganda, and Zambia each hold additional authority over nursing work and labor matters.
Part II

20 Journal of Nursing Regulation
Data on the regulatory body that governs the nursing profession in the Central African Republic, Comoros, and Congo are un-
available. Togo is unique as there is no official NRB; however, the National Association of Nurses of Togo is an important resource for
nurses, members of the association, and authorities. Procedures are underway for the creation of the National Order of Nurses of Togo,
which will serve as the official NRB.
NRB Mandate/Mission
All African jurisdictions report that the mandate of their NRB includes public protection. For 15 of these countries (Benin, Botswana,
Burkina Faso, Côte d’Ivoire, Djibouti, Egypt, Ethiopia, Gabon, Gambia, Libya, Mali, Mauritania, Niger, Rwanda, and South Africa),
public protection is the only mandate of the NRB. In 23 countries (Burundi, Cameroon, Cape Verde, Congo, Eswatini, Ghana, Guinea,
Kenya, Lesotho, Liberia, Madagascar, Malawi, Mauritius, Morocco, Mozambique, Namibia, Nigeria, Seychelles, Eswatini, Tanzania,
Togo, Uganda, Zambia, and Zimbabwe), the regulatory body also states that promotion of the nursing profession is an additional man
-
date. Regulatory bodies in 11 countries (Cape Verde, Congo, Guinea, Kenya, Madagascar, Mozambique, Nigeria, Seychelles, Tunisia,
Uganda, and Zambia) have additional mandates related to workforce or labor and union concerns.
Composition of NRBs
For those African jurisdictions for which data are available related to the size of the regulatory body (n = 19), the average size of the
regulatory body is 15 members (Table 1). The smallest regulatory bodies in Africa are the Order of Nurses of Mozambique and the
Nurses and Midwives Council of Malawi, each consisting of five members. The largest African regulatory body is the 25-member
Nursing Council of South Africa.
TABLE 1
Number of Members on Nursing Regulatory Bodies in Africa
Country Number of Members
Malawi 5
Mozambique 5
Eswatini 9
Namibia 10
Ghana 11
Seychelles 13
Tanzania 13
Kenya 15
Rwanda 15
Zimbabwe 15
Country Number of Members
Madagascar 16
Liberia 17
Zambia 17
Botswana 18
Mauritius 19
Uganda 19
Nigeria 22
Lesotho 23
South Africa 25
In 12 of the African regulatory bodies, those serving on the regulatory body are nominated by their professions. In Côte d’Ivoire,
South Africa, Eswatini, Uganda, and Zambia, those serving on the regulatory body are appointed by the government, while in Botswana
and Madagascar, the regulatory body is elected. In the remaining countries, the regulatory body consists of a combination of elected and
appointed members, or, in the case of six countries, include ex-officio members.
Data related to the composition of the regulatory body were available for 36 African countries. Twenty-five of these have nurses
serving on their regulatory bodies. Of those 11 that do not include nurses on their NRBs, 9 are in countries where the Ministry of Health
oversees nursing regulation, and the NRB is comprised of public servants who may not belong to a health profession. In Morocco and
Tunisia, the NRB includes physicians, but information is not available on who else serves. Physicians also serve alongside nurses in 9
additional African NRBs. Thirteen African NRBs include members of the public as well.
Apart from these more common representatives, some countries have additional requirements for representatives in their nursing
regulatory body (Table 2).

www.journalofnursingregulation.com 21Volume 10
•
Special Issue
•
January 2020
TABLE 2
Representatives Required in African Countries Nursing Regulatory Boards
Required Representatives Countries
Technical advisors Burkina Faso
Health inspectors Burkina Faso
Health facility representatives Burkina Faso
Educators Burkina Faso, Gambia, Namibia, South Africa
Professional association Gambia
Legal professional Gambia, Namibia, South Africa
Accountant South Africa
Pharmacist Burkina Faso, South Africa
Nurses from specific specialties Mauritius, South Africa
Few African countries specify additional qualifications for their regulatory body representatives. Ethiopia has the most stipulations,
specifying that those serving must be of good moral character and mental health, with no addictions or criminal history. Gambia re
-
quires each region be equally represented and the involvement of the professional association. Conversely, Mozambique does not allow
its regulatory body members to take part in the professional associations. Mauritius and Liberia both set a minimum number of years
of experience in nursing before someone can serve, while Eswatini requires a master’s in nursing.
Licensure and Registration Requirements to Practice
The licensure and registration responsibilities of each NRB body vary according to jurisdiction. Several African countries have additional
requirements for a nurse to be authorized to practice, beyond completion of education. Mauritius specifies the nurse must be a citizen
who has never been removed from the register in any country where he or she has practiced and is physically and mentally fit. Seychelles
sets a minimum age of 19 years for nurses.
Data were not always available as to practice requirements for nurses educated outside each African country. In some cases, profi
-
ciency in a specific language is required. For Ghana, South Africa, and Zimbabwe, English proficiency must be demonstrated prior to
authorization to practice. Tunisia requires French. Cape Verde specifies a language certification must be issued (the official language of
Cape Verde is Portuguese) and Madagascar specifies nurses must be able to communicate in the language of the patient (official languages
of Madagascar are French and Malagasy).
Most jurisdictions in Africa require a national examination after education is completed before a nurse is authorized to practice;
however, Cape Verde does not require examinations for authorization to practice in any nurse roles. There is no required national examina
-
tion for the RN, registered midwife, enrolled nurse, or community health nurse roles in Gambia. Mauritius does not require a qualifying
examination for its enrolled or assistant nurses, and Botswana does not have a qualifying examination for the psychiatric nurse role.
In general, registration is the means by which most nurses in Africa are authorized to practice. Djibouti, Guinea, Libya, Mali, and
Mauritania are exceptions in that they have a licensing process, while Ethiopia, Gambia, Lesotho, and Rwanda require both licensure
and registration. In Cape Verde, Mauritius, Niger, and Togo, nursing professionals are considered authorized upon completion of their
nursing education and receipt of diploma. This is also the case for midwives practicing in Gabon, as they are authorized to practice after
successful completion of education and training in midwifery. In Kenya, RNs must be registered in order to practice, while other types
of nurses are granted authority by license. The Liberian Board for Nursing and Midwifery allows graduate nurses (nurses who have taken
their examination but are not yet registered) to practice under the supervision of an RN while awaiting registration.
Once a nurse is registered and or licensed, a public database is the means by which a nursing professional’s credentials are verifiable.
Africa generally relies on paper-based databases. Only Cameroon, Congo, Gambia, Kenya, Lesotho, Mauritius, South Africa, Tunisia,
and Uganda have online systems. South Africa further restricts access to this information to employers.
Nurse Types and Titles
As far as categorizing nurse types in Africa, there are generally no more than three or four types per country, including a nurse, midwife,
specialized nurse, and nurse assistant (Table C1). Additionally, some jurisdictions designate specific specialty nurses (Table C2). Many
jurisdictions recognize some sort of mental health or psychiatric nurse. Other specialized nurse designations may include an ophthalmic
nurse, community health nurse/community nurse, reproductive health nurse, nurse anesthetist, master’s nurse, oncological nurse, theater
(surgical) nurse, nurse clinician, nurse practitioner, licensed practical nurse, or post-basic nurse. Ghana provides nine specialty nurse
type designations, including many of the types mentioned above, as well as a pediatric nurse and a critical care or perioperative nurse.

22 Journal of Nursing Regulation
Interestingly, a few African jurisdictions designate a unique title to what is commonly referred to as a midwife (Table C3). The
Cameroon Ministry of Public Health designates a qualified wise woman or a “qualified sage-femme” and Congo designates a wise
woman as midwives.
In most African countries, the lowest level of nurse recognized is usually referred to as an auxiliary nurse (Table C4). Data about
education requirements for this level of nurse were often unavailable.
Education
To commence education as a general RN in some African jurisdictions (Table 1 through 4), nearly all African NRBs require the comple-
tion of secondary education, usually specifying that 12th grade must be completed, a General Certificate of Education must be earned,
or certain ordinary level (“O” level) examinations must be passed. Ethiopia and Niger allow nursing education to begin after 10th grade,
although in Ethiopia, a prospective bachelor of nursing student must still complete 12th grade to commence education. In Tunisia, there
is no reported school requirement, but applicants must be aged at least 17 years. In Zambia, working for 3 years as a medical assistant
may stand in lieu of the secondary education requirement to begin nursing education at the regulatory body’s discretion. Burundi and
Cameroon require an entrance examination prior to studying nursing, while other jurisdictions in Africa set grade requirements in sci
-
ence (as in Gambia, Malawi, Mauritius, Nigeria, Rwanda, Tanzania, Zambia, and Zimbabwe), mathematics (Gambia, Nigeria, Rwanda,
and Zambia), or English (Gambia, Nigeria, Zambia, and Zimbabwe).
In African countries for which data are available, the mean length of a registered/general nursing program is 3.25 years. The vast
majority of jurisdictions have 3- to 4-year programs, although Burundi and Gambia state that the low end of this range may be 2 years
or 2.5 years, respectively.
In those African countries that recognize enrolled nurses (n = 9), education lasts 2 years. Information about what kind of secondary
schooling, if any, is required prior to beginning education as an enrolled nurse in African jurisdictions is limited. Tanzania specifies a
minimum grade in secondary science education for those wishing to study enrolled nursing. Zambia also specifies science and English
education and has a minimum age of 17 years. For Rwanda’s associate nurse role, 3 years of secondary school must have been completed
prior to beginning nursing education.
For those wishing to commence midwife education, African countries overwhelmingly require the completion of secondary
school, although a few specify a subject or grade requirement, scores on O Level examinations, or set a minimum age. The exceptions
are Botswana, Cameroon, Gambia, and Lesotho, where only practicing nurses can train for midwifery.
The average duration of education for midwives in Africa is 2.75 years. For the four jurisdictions where midwife roles require
prior education as a nurse, there are varying lengths of additional education required. Registered midwives in Botswana must take 2
additional years. The qualified wise women in Cameroon must take 3 additional years, while Gambia and Lesotho require less additional
education with 1.5 years and 1 year, respectively. For jurisdictions where students can enter directly into midwife programs, as little as
1 year of training (Namibia, Zambia) or as many as 4 years (Malawi, Mozambique) may be required. The Liberian-trained traditional
midwife completes training at the community level, the length of which is not specified.
TABLE 3
Educational Requirements for Internationally Educated Nurses in Africa
Country Requirements
Botswana, Gambia, Ghana, Lesotho, Malawi, South Africa,
Zimbabwe
Transcript
Botswana, Ghana, Mauritius, Zimbabwe References/testimonials
Cape Verde, Ghana, Lesotho, Liberia, Mauritius, Namibia, Uganda,
Zimbabwe
Verified authorization to practice in home country/good standing
Botswana, Cape Verde, Gambia, Kenya, Lesotho, Liberia, Mada
-
gascar, Malawi, Morocco, Namibia, Nigeria, Tunisia, Uganda,
Zimbabwe
Proof of completion of education/training
Gambia, Mauritius, South Africa Copy of license/certification from home country
Ghana, South Africa Marriage license if applicable
Ghana, Kenya (if needed), Seychelles (if needed) Additional examination
Ghana, Kenya, Namibia (if needed) Practical orientation
Guinea, South Africa Authorization to work in-country
Kenya Oral interview
Lesotho, Madagascar Curriculum Vitae
Liberia, Uganda Passed board examination in home country
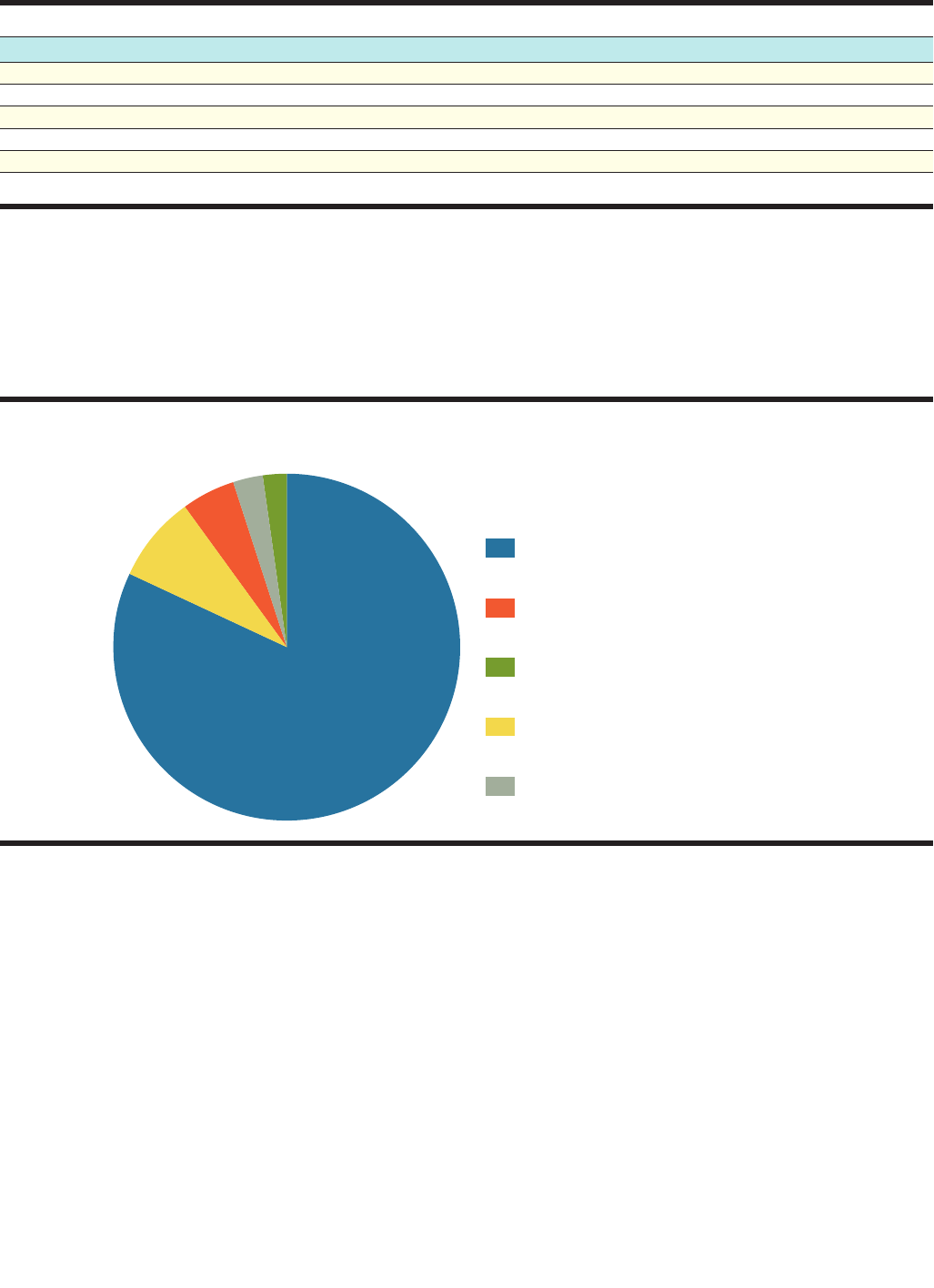
www.journalofnursingregulation.com 23Volume 10
•
Special Issue
•
January 2020
TABLE 3 (continued)
Country Requirements
Madagascar, Malawi, Mauritius, Nigeria Proof of morality
Madagascar, Tunisia Proof of physical fitness
Madagascar, Morocco, Tunisia Criminal history
Cape Verde, South Africa, Togo
a
Union/association affiliation
South Africa Enrollment at nursing school in-country
a
Nurses wishing to work in Togo must join the National Association of Nurses, as there is no dedicated government regulatory body.
Nursing Program Approval
The authority to approve nursing programs/schools is most commonly vested in NRBs, as 33 NRBs have authority over nursing educa-
tion in Africa (Figure 1). In Rwanda and South Africa, the approval of programs is shared jointly with each country’s respective higher
education authority. In five countries, the responsibility for approving programs is held elsewhere: (a) in Kenya and Togo, the minis
-
try of health is responsible; (b) in Ethiopia and Congo, the ministry of higher education is responsible; and (c) in Egypt, the General
Directorate of Technical Education for Health is responsible. Data were unavailable as to how the process is handled in the Seychelles.
FIGURE 1
Nursing Program Approval Authority in Africa
Regulatory Body
Jointly With Higher Education Authority
Ministry of Health
Higher Education Authority
No Data Available
8%
2%
5%
3%
82%
Continuing Competence
Continuing Competence within the nursing profession appears to be a requirement throughout approximately half of Africa, including
Benin, Botswana, Burkina Faso, Cameroon, Cape Verde, Eritrea, Ethiopia, Ghana, Guinea, Kenya, Lesotho, Liberia, Madagascar, Morocco,
Mozambique, Namibia, Nigeria, Rwanda, the Seychelles, Tanzania, Uganda, Zambia, and Zimbabwe. Many countries, however, do not
explicitly address continuing education in their regulations or nursing council websites. Jurisdictions address continuing competence
requirements differently. For example, the Nursing and Midwifery Council of Botswana and the Lesotho Nursing Council both require
nursing professionals to demonstrate continuing learning and submit completed continuing professional development booklets to the
Council for approval. The Ethiopian Health Professionals Council requires renewal of professional continuing competence every 5 years.
The Nursing and Midwifery Council of Ghana requires nursing professionals to participate in continued development of knowledge,
skills, and attitudes by participating in a minimum number of approved professional development activities (the minimum varies by
nurse type).
Practice
Overall, areas of authorized practice data vary across all nurse types in some African countries. Data related to specific areas of practice for
RNs are unavailable. Such is the case in Mali, Mauritania, Mozambique, Niger, Nigeria, the Seychelles, Eswatini, Uganda, and Zambia.

24 Journal of Nursing Regulation
in nine countries where data was available, nurses have authority to prescribe medications, refer patients, and diagnose illnesses, but in
varying circumstances and to varying degrees.
In Botswana, registered midwives, family nurse practitioners (NPs), and community health nurses may diagnose patients and refer
them for additional medical care. Both Botswanan RNs and psychiatric nurses have prescriptive authority; however, the medications
they can prescribe depend on the drug catalog. In Ghana, registered midwives and registered public health nurses may refer patients for
additional medical care. Nurses and midwives in Benin have prescriptive authority and may refer patients for additional medical care.
In addition, the Cameroon Ministry of Public Health grants ophthalmic nurses the authority to diagnose common eye problems and
refer patients for care. Nurses, midwives, and specialist nurses in Lesotho are authorized to make nursing diagnoses and refer patients
for additional medical care. In Namibia, nurses can prescribe medications under an issued license and administer standard prescribed
medicines and treatment. They may refer patients but may not diagnose illnesses. In Madagascar, nurses can prescribe medications within
legal limits, in addition to appropriate radiological or laboratory tests. They can also refer patients and diagnose illnesses. Similarly,
nurses in Malawi can prescribe iron tablets, malaria dosage, automatic transport ventilators, all nonprescription drugs, and some pre
-
scription drugs, while also maintaining authority to refer and diagnose. In Togo, certified nurses may prescribe medications including
antalgics, anti-inflammatories, vitamins, anti-anemic medications, antibiotics, anti-malarial medications, and anthelmintics; they are
also authorized to refer patients and diagnose illnesses.
Practice data for an RN in Tunisia are unavailable, but a Tunisian midwife (wise woman) has the authority to prescribe medica
-
tions and refer patients. In Cameroon, a qualified wise woman has the authority to refer patients for additional medical care. This type
of midwife has prescriptive authority only as necessary for obstetric purposes. Similarly, in Congo, a wise woman can refer patients as
necessary to the exercise of the profession and may diagnose pregnancies.
Discipline
Governing bodies in many jurisdictions have authority to take disciplinary measures against nursing professionals who violate standards
of professional conduct. In terms of discipline, the following actions are commonly taken in Africa: (a) suspension of practice, (b) removal
of name from register/refusal to register/restricted registration, (c) revocation or denial of license, (d) warnings, (e) practice probation,
(f) probation, (g) fine or civil penalty, (h) practice limitation with/without probation, (i) intensified supervision, (j) reprimand, and (k)
imprisonment. Kenya, Lesotho, and Liberia use additional disciplinary measures inclusive of the requirement of additional training and
education at the cost of the nursing professional.
Just as some jurisdictions offer a public registry of verified nursing professionals, some jurisdictions offer a public database where
disciplinary records of nursing professionals are freely available. Disciplinary records are available to the public in a limited number of
African countries, including Cameroon, Ethiopia, Gambia, Malawi, Morocco, South Africa, Uganda, and Zimbabwe. Jurisdictions where
such records are available in the same source as the registry of nurses include Cameroon, Ethiopia, Gambia, and Uganda. However, Ghana
and Malawi both hold disciplinary records of nursing professionals in a separate database, which is open to the public in the council
offices and available by inspection. In Morocco, records of sanctions are published in the National Bulletin. South Africa’s disciplinary
records against nursing professionals are stored in an online database, but the country is currently developing an integrated electronic
system to include human resources, finance, registration, and examinations, among other areas. This comprehensive system allows ac
-
cessibility of a nurse’s education and professional history from the training stage of nursing through retirement or death.
Most commonly, if an online database is not maintained, one can look to a jurisdiction’s national gazette or newspaper or file
a request with a respective nursing council office to inspect a nursing registry. Such is the case in Ethiopia, Ghana, Guinea, Liberia,
Mozambique, and the Seychelles. The Nursing and Midwifery Council of Botswana is in the process of establishing a system for public
access to its registry. Other African nations simply restrict registry access altogether, or their level of transparency related to monitoring
nursing professionals is unknown. Such is the case in Benin, Burkina Faso, Burundi, Cape Verde, the Central African Republic, Libya,
Mali, Mauritania, Namibia, Niger, Rwanda, Eswatini, Tanzania, and Togo, which accounts for 25% of Africa.

www.journalofnursingregulation.com 25Volume 10
•
Special Issue
•
January 2020
The Americas
T
he Americas are broken into the following regions: Canada, Caribbean nations and territories, Central America, Mexico, South
America, and the United States.
Canada
Canada comprises 13 provinces and territories including Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland and
Labrador, Nova Scotia, the Northwest Territories, Nunavut, Ontario, Prince Edward Island, Quebec, Saskatchewan, and the Yukon.
For the purposes of this report, the Northwest Territories and Nunavut was considered one jurisdiction. All Canadian jurisdictions are
members of the Canadian Free Trade Agreement (CFTA). Part of this agreement allows workers in a regulated profession, such as nurs
-
ing, who are authorized in one province to have their qualifications recognized throughout all Canadian provinces without completing
any additional requirements.
Regulation and Governance
Each Canadian province or territory maintains an independent nursing council, usually referred to as a nursing college, to regulate the
profession. Canada is distinct in that most jurisdictions maintain more than one NRB (Table 4). For example, in Alberta, there are three
regulatory bodies: the College and Association of Registered Nurses of Alberta, the College of Licensed Practical Nurses of Alberta,
and the College of Registered Psychiatric Nurses of Alberta. Public protection is the mandate for all Canadian territories/provinces,
and promotion of the nursing profession is also part of the mandate in New Brunswick, the Northwest Territories and Nunavut, Prince
Edward Island, Saskatchewan, and the Yukon.
TABLE 4
Canadian Nursing Colleges (Councils)
Province/Territory Nursing College
Alberta College and Association of Registered Nurses of Alberta
College of Licensed Practical Nurses of Alberta
College of Registered Psychiatric Nurses of Alberta
British Columbia British Columbia College of Nursing Professionals
Manitoba College of Registered Nurses of Manitoba
College of Registered Psychiatric Nurses of Manitoba
College of Licensed Practical Nurses of Manitoba
New Brunswick Nurses Association of New Brunswick
Association of Licensed Practical Nurses
Newfoundland and Labrador Association of Registered Nurses of Newfoundland and Labrador
College of Licensed Practical Nurses of Newfoundland and Labrador
The Northwest Territories and Nunavut Registered Nurses Association of the Northwest Territories and Nunavut
Nova Scotia College of Registered Nurses of Nova Scotia
College of Licensed Practical Nurses of Nova Scotia
Ontario College of Nurses of Ontario

26 Journal of Nursing Regulation
TABLE 4 (continued)
Province/Territory Nursing College
Prince Edward Island College of Registered Nurses of Prince Edward Island
College of Licensed Practical Nurses of Prince Edward Island
Quebec College of Nurses of Quebec
Saskatchewan Saskatchewan Registered Nurses Association
Saskatchewan Association of Licensed Practical Nurses
Registered Psychiatric Nurses Association of Saskatchewan
The Yukon Yukon Registered Nurses Association
Each NRB comprises both nurses and public members, and Nova Scotia includes one nonvoting student member. The number
of NRB members ranges from seven in Quebec and the Yukon to 39 members in Ontario. Most NRBs require nurses to be actively
registered or licensed and in good standing to serve as a member. British Columbia, Quebec, and the Yukon, require their representa
-
tives to be residents of the province. British Columbia places a few more requirements on those serving, specifying they must not have
any insolvency, unprofessional conduct (in practice or in public service), or affiliation with a nursing professional organization. Prince
Edward Island’s regulatory bodies conduct a criminal history background check on those serving.
The responsibilities of all regulatory bodies throughout Canada include licensing and registering of nurses, administering nursing
laws and regulations, making scope of practice decisions, and disciplining nurses. All but Saskatchewan include creating legislation as
a governance power.
The NRBs have the authority to require a national examination for regulation/licensure as well as the authority to approve nurs
-
ing schools/programs. However, the Yukon does not have a school of nursing for RNs or NPs. As a result, all RNs or NPs in the Yukon
have obtained their nursing education in another jurisdiction.
Licensure and Regulation Requirements to Practice
In Canada, most jurisdictions authorize nurses to practice via registration, if not licensure. Alberta, British Columbia, Manitoba, New
Brunswick, the Northwest Territories and Nunavut, Ontario, Prince Edward Island, Saskatchewan, and the Yukon all require registration.
Newfoundland and Labrador, Nova Scotia, and Quebec issue nursing licenses. Once registered or licensed, a public database is typically
the means by which a nursing professional’s credentials are verifiable. Today, all Canadian jurisdictions except the Yukon maintain an
online, publicly accessible database. A language proficiency examination is required in all Canadian jurisdictions for nurses applying
for licensure/registration from another country. Additionally, some Canadian regulatory bodies report that NPs may require additional
authorization to prescribe certain medications. Prince Edward Island also requires liability insurance.
Nursing professionals in all Canadian jurisdictions must complete their education and other requirements, including a national
examination, before they may be registered or licensed. Most Canadian jurisdictions administer the NCLEX-RN examination for
registered nurses, the Canadian Practical Nurse Registration Examination (CPNRE) for practical nurses, and specialty examinations
for additional nursing roles, including the Registered Psychiatric Nurses of Canada Examination (RPNCE). (The exception is Quebec,
which offers its own examinations).
International nurses applying for licensure/registration in all Canadian jurisdictions are required to apply to the National Nursing
Assessment Service to be assessed for the comparability of their nursing education to the Canadian system. The national service provides
results to the appropriate provincial regulatory body, and a determination is made by the provincial body whether to license or register
in that province.
Nurse Types and Titles
There are generally four nurse types per province or territory, including RNs, licensed practical nurses (LPNs), NPs, and registered
psychiatric nurses (Tables C5 and C6). New Brunswick recognizes four additional nurse types, including public health nurses, clinical
nurse specialists, community health nurses, and private duty nurses (Table C6).
Education
The nursing education program requirements for the Canadian jurisdictions are presented in Tables C5 and C6.
Continuing Competence
All of Canada requires continuing competence. Specifically, British Columbia requires RNs to work a minimum number of practice
hours (1,125 hours over 5 years); complete a confidential self-assessment of their practice using applicable nursing council standards of

www.journalofnursingregulation.com 27Volume 10
•
Special Issue
•
January 2020
practice; seek and receive peer feedback (if they were engaged in practice during the previous year); develop and implement a learning
plan based on their self-assessment and peer feedback; and evaluate the impact of their learning on their practice.
The New Brunswick Nursing Councils and the majority of other Canadian provinces and territories that require self-assessment
state that nurses need a learning plan and evaluation to satisfy continuing competence, which may include: (a) seeking peer feedback;
(b) reading articles and/or textbooks; (c) networking and consulting with experts in a nursing facility; (d) shadowing an expert nurse; (e)
attending clinical practice rounds, seminars, in-services or workshops; (f) watching a video; (g) attending or participating in a clinical
case presentation; (h) enrolling in continuing education courses; (i) attending conferences; (j) completing certification in one’s specialty
area; and (k) mentoring a peer.
Practice
In Alberta, RNs may only prescribe medications from an approved list and may also refer patients. In British Columbia, they may
prescribe medications in accordance with Schedule I of the Drug Schedules Regulation for the purpose of treating certain illnesses and
disorders. They may also make diagnoses, but are restricted from referring patients. In most Canadian jurisdictions, NPs are authorized
to prescribe medications, diagnose illnesses, and refer patients (Table 5).
TABLE 5
Nursing Practice Authority in Canada by Jurisdiction
Province/Territory Nurse Type Prescriptive Authority Diagnosis Referral to Other Services
Alberta LPN No No data No
Psychiatric nurse No No data No
RN Yes; may only
prescribe medications
from an approved list.
No data Yes
NP Yes No data Yes
British Columbia LPN Yes Yes
RN Yes Yes
Registered psychiatric nurse Depends Yes Yes
NP Yes Yes Yes
Manitoba LPN No data No data No data
RN No Yes Yes
Registered psychiatric nurse No No data No data
NP Yes No data Yes
New Brunswick LPN No data No data No data
RN No No No
NP Yes Yes Yes
Registered psychiatric nurse No No No
Public health nurse No data No data No data
Clinical nurse specialist No data No data No data
Community health nurse No data No data No data
Private duty nurse No data No data No data
Newfoundland and
Labrador
LPN No data No data No data
RN No Yes, nursing
diagnosis only
Yes, in a limited capacity
NP Yes Yes Yes
Nova Scotia LPN No No No
RN No Yes, nursing
diagnosis only
Yes
NP Yes Yes Yes
Northwest Territories
and Nunavut
LPN No No data No
RN No No data No
NP Yes No data Yes
Ontario Registered practical nurse No No data No
RN No No data No
NP Yes No data Yes

28 Journal of Nursing Regulation
TABLE 5 (continued)
Province/Territory Nurse Type Prescriptive Authority Diagnosis Referral to Other Services
Prince Edward Island LPN No data No data No data
RN No data No data No data
NP Yes Yes Yes
Quebec RN Yes Yes No
NP Yes Yes Yes
Saskatchewan LPN No No No
Registered psychiatric nurse No No No
RN No No No
RN (additional authorized practice) Yes Yes Yes
NP Yes Yes Yes
Yukon RN No No No
NP Yes No Yes
Note. LPN=licensed practical nurse; NP=nurse practitioner; RN=registered nurse.
Discipline
In terms of discipline, the following actions are commonly taken in Canada: (a) censure, (b) cease and desist orders, (c) reprimand, (d)
suspension of license or registration, (e) remediation, (f) warnings, (g) fine or civil penalty, (h) practice limitation with or without proba
-
tion, (i) probation, (j) assessment of costs, (k) surrender of license, (l) revocation or denial of license, (m) supervised practice (which may
have time limitations and performance review requirements), (n) community service, and (o) citation orders.
As most countries incorporate a nursing professional’s disciplinary history into their nursing registry, Canada also maintains a great
degree of transparency related to its nursing professionals. Disciplinary records are available to the public in Alberta, British Columbia,
New Brunswick, Nova Scotia, Ontario, and Quebec. Information related to the availability of disciplinary records is unavailable in
Manitoba, the Northwest Territories and Nunavut, Prince Edward Island, and the Yukon. Saskatchewan restricts disciplinary data for
registered psychiatric nurses but grants public access to disciplinary records for other nurse types, including LPNs. The nursing councils
in Newfoundland and Labrador restrict nursing disciplinary records altogether.
The Caribbean Community (CARICOM)
The Caribbean region comprises numerous islands in the Caribbean Sea off the east coast of Central America and north coast of South
America, as well as some coastal countries on continental Central and South America, namely, Belize, Suriname, and Guyana, that
are culturally connected to the island region. The majority of jurisdictions in this region participate to some degree in the Caribbean
Community (CARICOM) compact. The jurisdictions are organized here as CARICOM member states, associate member states, and
non-CARICOM nations.
CARICOM Member States
CARICOM is comprised of Antigua and Barbuda, Bahamas, Barbados, Belize, Dominica, Grenada, Guyana, Haiti, Jamaica, Montserrat,
Saint Kitts and Nevis, Saint Lucia, Saint Vincent and the Grenadines, Suriname, and Trinidad and Tobago.
Regulation and Governance
Regulatory bodies that govern and regulate nursing in CARICOM member states are most commonly national nursing councils, which
are independent from bodies that regulate other professions. Each nursing council consists of seven to 16 members (Table 6).
In Haiti and Suriname, a national Ministry of Health is the regulatory body that governs nursing and other health professions. In
Haiti, the Department of Nursing within the Ministry of Health and Population holds nursing regulatory authority. This body holds
the power to license nurses, ensure adequate financing, promote both public protection and the nursing profession, handle nursing work
force and labor issues, ensure national and international standards, take disciplinary action, administer nursing laws and regulations,
make decisions on nursing scope of practice, and approve nurse training and education programs. In Suriname, the Ministry of Health
has regulatory authority regarding nursing and promotes public protection, administer nursing laws and regulations, make decisions
on nursing scope of practice, participate in disciplinary action, approve nurse training programs, and create nursing legislation.

www.journalofnursingregulation.com 29Volume 10
•
Special Issue
•
January 2020
Guyana and Suriname are unique in that both jurisdictions are also associate members of the Southern Common Market
(MERCOSUR), which is a regional compact of South American nations that collaborate to generate business and development of the
region. As associate members, Guyana and Suriname have entered into agreements with member states regarding economic integrations
in Latin America; however, they follow CARICOM nursing standards and recommendations.
Montserrat is a British territory; it is autonomous, and its constitution is provided for under the United Kingdom. As such,
citizens of Montserrat are also British citizens. The Montserrat Nurses and Midwives Board is the governing body for nursing; however,
the British Crown retains the power of ultimate judicial appellate review.
Most CARICOM member state nursing councils share a common mandate to promote public protection and the nursing profes
-
sion. Antigua and Barbuda, Haiti, and Jamaica oversee nursing workforce, labor, or union issues. Haiti also incorporates a mandate
to ensure adequate financing. Each CARICOM member state nursing council has the authority to license nurses, require a national
examination to practice nursing, administer nursing laws and regulations, make decisions on nursing scope of practice, and participate
in disciplinary action. Notably, only Belize, Dominica, Saint Lucia, Suriname, and Trinidad and Tobago can extend authority to either
create nursing legislation or participate in its creation.
Composition of the NRB
The NRBs of Antigua and Barbuda, Bahamas, and Grenada, and St. Lucia are composed of both nurses and physicians. Grenada also
includes a registered midwife and a nursing assistant among its council members. Dominica and Montserrat include nurses, physicians,
and public members. Barbados includes a mix of nurses, Minister appointees, ex officio members, and a member of the general public.
Belize also includes public representatives on its nursing council.
The NRBs of Antigua and Barbuda, Guyana, Saint Lucia, and Trinidad and Tobago are a mix of appointed and elected represen
-
tatives. In Antigua and Barbuda, at least two members must be RNs. The Bahamas and Saint Lucia nursing councils include medical
practitioners among their members. Jamaica’s Minister of Health appoints the nursing council members with recommendations from
professional nursing/midwifery organizations. Grenada also includes a registered midwife and a nursing assistant among its council
members. Dominica and Montserrat include nurses, physicians, and public members. Barbados includes a mix of nurses, Ministry ap
-
pointees, ex officio members, and a member of the general public. Belize also includes public representatives on its nursing council.
TABLE 6
Number of Members on Nursing Regulatory Bodies in Caribbean Community Member States
Jurisdiction Number of Members
Antigua and Barbuda 7
Dominica 7
Montserrat 7
Saint Lucia 9
Bahamas 10
Grenada 12
Belize 13
Barbados 15
Jurisdiction Number of Members
Guyana 15
Jamaica 15
Trinidad and Tobago 16
Haiti Not available
Saint Kitts and Nevis Not available
Saint Vincent and the Grenadines Not available
Suriname Not available
Licensure and Registration Requirements to Practice
CARICOM member states grant authorization to practice nursing via registration or licensure. Authorization is granted after the nursing
professional has completed the education and training requirements set forth by CARICOM, as well as the respective nursing council
or Ministry of Health. The majority of member states recognize authority to practice through registration; however, Grenada and Saint
Lucia authorize practice by licensure. Haiti recognizes authority to practice by both licensure and registration.
Nurse Types and Titles
There are generally four-to-six nurse types overall per jurisdiction, including that of an RN, NP, midwife, and nursing assistant.
Education
CARICOM requires a 4-year bachelor of science in nursing degree for registration or licensure. Additional education and training re-
quirements vary among nursing professions (Table C7).

30 Journal of Nursing Regulation
Many member states (Dominica, Grenada, Guyana, Jamaica, Montserrat, Saint Lucia, and Saint Vincent and the Grenadines)
grant their nursing councils authority to approve nursing education programs. Although the national nursing councils in Barbados and
Trinidad and Tobago have broad authority, authorization of nurse education programs is approved by each Ministry of Health.
Continuing Competence
Following entry into practice, continuing competence is required by a majority of CARICOM member states. This requirement must
be completed either biannually, or by the time of license renewal. In the Bahamas, for instance, it is necessary for a nursing professional
to complete educational contact hours in order to renew their professional license.
Practice
The authorized areas of practice within the nursing profession vary between member states. For example, Dominican RNs may diagnose
and refer patients and have prescriptive authority. Specifically, they may prescribe oral, intramuscular, and intravenous medications.
Likewise, RNs in Montserrat are allowed prescriptive authority; however, they may only prescribe simple analgesics, mild antacids, vi
-
tamins, and anti-flatulent drugs. In Haiti, pediatric nurses may diagnose patients. In Trinidad and Tobago, midwives may refer patients
for additional medical care, while in the Bahamas and Barbados, they are authorized to prescribe dietary supplements.
Discipline
Nursing professionals in CARICOM member states are held to a code of ethics or standards and are expected to execute their professional
roles in a manner consistent with the code. Most CARICOM NRBs implement certain disciplinary actions and measures to nursing
professionals who have broken the code. Disciplinary measures that some member states take include a fine or civil penalty, license
suspension, surrender of license, license revocation, community service, continued training, or imprisonment. Regulatory bodies may
also issue a censure, reprimand, warning, denial of a license, or the removal of a professional’s name from the nursing register.
Some member states have made the disciplinary records of such individuals either publicly available or available upon request.
The Bahamas, Barbados, and Jamaica publish this information in their national gazette or newspaper. Belize, Haiti, and Trinidad and
Tobago make such information available only upon request.
Associate Member States
In addition to the 15 member states that comprise CARICOM, there are five associate member states: the British Virgin Islands, Anguilla,
Bermuda, Cayman Islands, and Turks and Caicos Islands.
Regulation and Governance
All five CARICOM associate member states are also British territories, and each state’s constitution is provided for under the United
Kingdom. As such, citizens of each associate member state are also citizens of the United Kingdom. Although each associate members’
governing body may regulate nursing, the British Crown retains the power of ultimate judicial appellate review.
The regulatory bodies that govern and regulate nursing in all associate member states are national nursing councils, which are
independent from the regulation of other professions. Each nursing council consists of five or more members (Table 7).
TABLE 7
Number of Members on Nursing Regulatory Bodies in Caribbean Community Associate
Member States
Associate Member Jurisdiction Number of Members
Turks and Caicos Islands 5
Cayman Islands 6
British Virgin Islands 7
Associate Member Jurisdiction Number of Members
Bermuda 9
Anguilla Not available
All CARICOM associate member nursing councils have a mandate to promote public protection and the nursing profession.
Largely, these regulatory bodies have the authority to license nurses, require a national examination to practice nursing, administer
nursing laws and regulations, make decisions on nursing scope of practice, and participate in disciplinary action. The Anguilla Nursing
Council holds the additional power to create legislation, while the mandate of the British Virgin Islands Nurses and Midwives Council
allows for any other activity that may be required under the Nurses and Midwives’ Act. Additionally, the British Virgin Islands and
Anguilla hold the power to approve nurse education and training programs.

www.journalofnursingregulation.com 31Volume 10
•
Special Issue
•
January 2020
In contrast, the Bermuda Nursing Council holds many of the powers mentioned above except licensing authority and the power
to approve nursing education and training programs. Instead of issuing a national license to practice in the nursing profession, Bermuda
allows authority to practice by endorsement. In this case, the nursing professional should have successfully passed a qualifying examina
-
tion in another jurisdiction and must subsequently petition the Bermuda Nursing Council for authorization to practice in Bermuda.
Nurses who have been trained in Bermuda will sit for the NCLEX in New York.
Licensure and Registration Requirements to Practice
Apart from Bermuda, who allows authority to practice by endorsement, as discussed above, associate member states of CARICOM
grant authorization to practice nursing by way of registration or by combination of licensure and registration. Authorization is granted
after the nursing professional has completed the education and training requirements set forth by CARICOM, as well as the respective
nursing council. For example, nursing professionals in the British Virgin Islands and Turks and Caicos Islands need only be registered
in order to practice the profession. On the other hand, nursing professionals in the Cayman Islands and Anguilla are required to be both
licensed and registered.
The names of nursing professionals authorized to practice in associate member states are found in a nursing registry. In all associ
-
ate member states, this registry is available to the public and can be found online, in the national newspaper, or by visiting the office
of the respective nursing council.
Nurse Types and Titles
CARICOM associate member states employ standard titles and language. There are generally four to six nurse types per jurisdiction,
including RNs, nursing assistants, NPs, and midwives (Table C8).
Education
Associate member states follow CARICOM nursing education standards. These standards mandate that for nurses to be registered or
licensed with a bachelor of science in nursing degree, they shall have completed 4 years of training and education. Additional education
and training requirements vary regarding nursing professions (Table C8).
Continuing Competence
Following entry into practice, continuing competence is regularly required by all associate member states and for many nurse types.
This requirement is usually biannual or by the time of license renewal.
Practice
Authorized practice areas within the nursing profession varies between associate member states. In Bermuda, an advanced practice nurse
has authority to refer patients for additional medical care but does not have authority to prescribe.
Discipline
Nursing professionals of CARICOM associate member states are held to a code of ethics or standards and are expected to execute their
professional roles in a manner consistent with the code. All regulatory bodies of associate member states implement certain disciplinary
actions and measures to nursing professionals who have broken the code. Disciplinary measures that some associate member states take
include the order of a fine or civil penalty, license suspension, summary suspension, surrender of license, license revocation, continued
training, or imprisonment. Regulatory bodies may also issue a censure, reprimand, warning, denial of a license, license surrender, limit
on professional practice, denial of license renewal, or the removal or cancellation of a professional’s name from the nursing register. Some
associate member states have made the disciplinary records of such individuals publicly available, including the British Virgin Islands,
Cayman Islands, and Turks and Caicos Islands. These records may be found either in the respective national gazette or newspaper or
other forms.
Non-CARICOM Nations
There are additional Caribbean nations outside of CARICOM. The following analysis focuses on Aruba, Cuba, Martinique, and the
Dominican Republic, which are independent of CARICOM. For jurisdictional convenience, the Caribbean jurisdictions of the U.S.
Virgin Islands and Puerto Rico are included in the analysis of the United States.
Regulation and Governance
The National Association of Nurses in Cuba and the National Council Order of Nurses in Martinique are the regulatory bodies that
govern and regulate nursing in those islands. They are independent from bodies that regulate other professions. These regulatory bod
-
ies hold the power to license nursing professionals, administer laws, promote public health and the nursing profession, and discipline

32 Journal of Nursing Regulation
nurses. Cuba’s National Association of Nurses holds additional powers to create legislation, make decisions on nursing scope of practice,
contribute to nursing research, and participate in educational concerns in conjunction with its Ministry of Public Health.
Martinique is an overseas department of France. As such, Martinique is a part of the European Union (EU) and its citizens are also
French citizens. Martinique’s National Council Order of Nurses, through its Regional Health Authority, is an independent governing
body, yet it follows French nursing regulations under the French Ministry of Solidarity and Health.
Larger agency bodies govern the nursing profession in Aruba and the Dominican Republic. Aruba is an overseas territory of the
Netherlands and its citizens are also citizens of the Netherlands. However, Aruba is not a member of the EU and maintains its own
laws. As such, the Ministry of Tourism, Public Health, and Sports regulates the nursing profession. The Ministry of Public Health and
Social Assistance regulates nursing in the Dominican Republic and is composed of ex officio members, public officials, and medical/
health professionals.
The powers of the regulatory bodies in both Aruba and the Dominican Republic include: (a) creating legislation, (b) taking disci
-
plinary action, (c) administering nursing laws and regulations, (d) promoting public protection and the nursing profession, (e) making
decisions on nursing scope of practice, and (f) licensing nursing professionals. In addition, the Dominican Ministry of Public Health
and Social Assistance handles nursing profession labor and workforce issues, as well as matters in continuing competence.
No data are currently available on the number of members in the NRB of the non-CARICOM members.
Licensure and Registration Requirements to Practice
Each of the non-CARICOM jurisdictions grant authorization to practice nursing via registration or licensure. Notably, Aruba grants
authorization to practice by the issuance of a Certificate of Competence. Authorization is granted after the nursing professional has
completed the education and training requirements set forth by the respective regulatory body.
As with Caribbean nations that participate in CARICOM, the names of nursing professionals in Aruba, Cuba, Martinique, and the
Dominican Republic who can practice are found in a nursing registry. This registry may be available online, in each nation’s newspaper,
inside the office of the governing body, or a combination of all the above. Uniquely, the registry of nursing professionals of Martinique
is available through the French online nursing registry. The Dominican Republic allows access to its registry of nursing professionals
by request through the Ministry of Public Health and Social Assistance.
Nurse Types and Titles
Only three non-CARICOM nations reported data on nurse types, and they used simple titles and standard language. There are generally
no more than three types per jurisdiction, including nurses, doctors of nursing, and midwives (Table C9).
Education
Professional education and training requirements vary in Aruba, Cuba, and Martinique (Table C9). For instance, a nurse may be autho-
rized to practice in Aruba and Martinique after only 3 years of training, whereas a nurse with a bachelor of science in nursing in Cuba
is subject to 5 years of education and training.
Continuing Competence
The Dominican Republic includes the promotion of continuing education/competence among its regulatory body mandates, though
data are lacking on its specific continuing competence requirements. Nursing professionals in Martinique must comply with continu
-
ing competence requirements, which stipulate the professional must justify nurse training, evaluation, analysis, and improvement in
nursing practices and risk management over 3 years.
Practice
The areas of practice within the nursing profession varies between all jurisdictions. In Aruba, midwives have authority to diagnose
patients and refer them for additional medical care. They also hold limited prescriptive authority, as they may prescribe medication if a
doctor is unable to administer or prescribe the necessary medication. Midwives in Martinique also hold limited prescriptive authority.
They may prescribe vaccinations for women and newborns under measures as determined by decree. In addition, they may also prescribe
drugs of a therapeutic class appearing on a list fixed by the French Ministry of Solidarity and Health. Nurses in Martinique may refer
patients for additional care. They also have the authority to renew prescriptions that are less than 1 year old and that comport with a list
set by the Ministry of Solidarity and Health. Nurses in Martinique may prescribe nicotine supplements. In Cuba, nurses may diagnose
patients and refer them for additional medical care. They also have prescriptive authority; however, that authority varies depending on
the specific type of specialist nurse. Licensed nurses in Cuba may diagnose patients and refer them for additional care.
www.journalofnursingregulation.com 33Volume 10
•
Special Issue
•
January 2020
Discipline
Similar to CARICOM member and associate member states, most nursing professionals in other non-CARICOM nations are held to
a code of ethics or standards and are expected to execute their professional roles in a manner consistent with the code. Disciplinary
measures that Aruba, Martinique, and the Dominican Republic take include the issuance of fines or civil penalties and the denial of
professional certificates or licenses. Additional disciplinary measures taken by Martinique and the Dominican Republic include an order
of reprimand, warnings, sanctions, and suspensions. Martinique disciplinary measures may also include imprisonment or a prohibition
or limitation on the authorization to practice nursing, whereas the Dominican Republic may also order any other sanction consistent
with that nation’s Trujillo Public Health Code. Martinique makes its disciplinary records of nursing professionals publicly available
through its National Council of Nurses and its Automated Directory of Health Professionals database.
Central America
Central America includes Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua, and Panama. Currently, these countries are not
members of any regional compacts or mutual agreements that influence the nursing profession. The Central American nation of Belize
is included among the CARICOM member states due to its membership therein, and is not discussed in this section. Information for
Panama was not publicly available; thus, Panama is not in this report.
Regulation and Governance
In terms of nursing governance, both independent NRBs and larger agencies regulate the nursing profession throughout Central America.
Costa Rica and Honduras are governed by independent bodies, while El Salvador, Guatemala, and Nicaragua are regulated by their
respective Ministry of Health organizations.
The mandates of most of the Central American NRBs include public protection, promotion of the profession, and/or workforce,
labor, or union issues. However, El Salvador identifies professional practice surveillance as its primary mandate.
Except for Honduras, all other Central American NRBs have the authority to require and designate a required national examination
to practice nursing. All NRBs also have the authority to approve nursing schools/programs; however, El Salvador works in conjunction
with its Ministry of Education to approve nursing schools and programs, and Honduras reserves this authority entirely to its Higher
Education Council (Consejo de Educacion Superior).
The majority of the NRBs in this region are responsible for administering nursing laws and regulations, making decisions about
scope of practice, and disciplining nurses.
Nurses compose the NRBs for Costa Rica, El Salvador, and Honduras, whereas public servants are regulatory body members in
Guatemala. There is no information available for the composition of the Nicaraguan NRB. The number of members serving on each
NRB is shown in Table 8.
El Salvador requires that all members or alternate members of the NRB are Salvadoran, are citizens older than 30 years, are profes
-
sionally trained with practice experience, live in the country for 5 years prior to their appointment or election, and are “of recognized
morality.” Members are elected in Honduras and Costa Rica, but data are lacking about requirements to serve.
TABLE 8
Number of Members on Nursing Regulatory Bodies in Central America
Country Number of Members
Costa Rica 8
Honduras 10
El Salvador 14
Country Number of Members
Guatemala Not available
Nicaragua Not available
Licensure and Registration Requirements to Practice
All Central American NRBs are responsible for licensing/registering nurses. Registration and licensure are both required in El Salvador,
whereas Guatemala and Nicaragua only require registration. Costa Rica and Honduras issue licenses to authorized nursing professionals.
Costa Rica, El Salvador, and Nicaragua require a national examination after education is completed, whereas Honduras does not.
There are no data available for Guatemala.
Once registered and/or licensed, a public database is the means by which a nursing professional’s credentials are verifiable. Only
Guatemala and Nicaragua utilize an online, public database. El Salvador and Honduras restrict all access to nursing-related informa
-

34 Journal of Nursing Regulation
tion, including disciplinary actions. It is not clear what level of transparency Costa Rica maintains concerning information related to
its nursing professionals.
Nurse Types and Titles
As far as categorizing nurse types, there are generally no more than four nurse types per jurisdiction and these types include nurses,
midwives, specialized nurses, and nurse assistants. Midwifery is recognized and regulated by registration in Nicaragua, and Guatemala
incorporates educational levels into its nurse titles (Table C10).
Education
There is limited education data available for the duration and program entry requirements for all nurse education programs in Central
America. The bachelor of nursing program in El Salvador and primary nurse program in Honduras are 5 years in duration, whereas the
RN program in Nicaragua is 3 years in duration to read in America (Table C10).
Continuing Competence
Continuing Competence are required in Costa Rica, Guatemala, and Nicaragua, but not in El Salvador and Honduras.
Practice
Practice data for nurses vary across Central America and are unavailable in Guatemala and Nicaragua. Nurses in Honduras are authorized
to diagnose illnesses and refer patients. It is not clear whether Honduran nurses can prescribe medications. In contrast, nurses in Costa
Rica are completely restricted from performing any of those functions. El Salvador grants nurses limited prescribing rights (including the
authority to prescribe supplemental vitamins, anti-parasitics, and antipyretics) and full authority to diagnose illnesses and refer patients.
Discipline
Past or current disciplinary actions are publicly accessible as part of a nursing registry in those countries that have one. In terms of
discipline, the following actions are commonly taken in Central America: (a) suspension, (b) revocation, (c) warnings, (d) fine or civil
penalty, (e) admonishment, (f) reprimand, (g) surrender or denial of license, (h) removal or denial of name from register, and (i) practice
limitations.
Mexico
The United Mexican States (Mexico) is a federal republic composed of 31 states and the Federal District. The nursing profession is
regulated at the federal level.
Regulation and Governance
The Mexican regulatory body for nursing is the Ministry of Health, which is a larger agency that regulates many professions and is
mandated to provide public protection and promote the nursing profession.
The Ministry of Health in Mexico is responsible for administering nursing laws and regulations, making decisions about scope
of practice, creating nursing legislation, and disciplining nurses. Information is not publicly available as to how large the Mexican
Ministry of Health is or what qualifications are required to serve on this regulatory body. Nursing education programs are approved by
the Secretary of Health and Secretary of Public Education.
Licensure and Registration Requirements to Practice
Mexico recognizes authorized nursing professionals who have completed their mandatory education and other requirements in the
granting of nursing licensure and/or registration. Mexico issues licenses to nursing professionals and uses an online, public database for
verifying a nursing professional’s credentials.
The Centro Nacional para la Evaluación de la Educación Superior (CENEVAL) examination is required for licensed nurses (a
title similar to an RN or general nurse) to practice in Mexico. In addition to educational requirements, graduation examinations are
required for master’s and doctoral nurses. Additionally, the doctoral nurse must pass a thesis defense. No examinations are required for
the remaining nursing types. Nurses coming to Mexico from another country must pass a language proficiency examination.
Nurse Types and Titles
There are seven types of nurses in Mexico that are primarily identified by the level of education required for licensure (Table C11).

www.journalofnursingregulation.com 35Volume 10
•
Special Issue
•
January 2020
Education
In Mexico, nursing education programs are approved by the Secretary of Health and Secretary of Public Education. See Table C15 for
requirements for entry into nursing programs and length of nursing education.
Continuing Competence
Mexico does not mandate continuing competence.
Practice
Authorized areas of practice varies based on nursing role and educational level. Table 9 demonstrates the variation in scope of practice
for the seven types of nurses in Mexico. The majority of nurses have some level of prescriptive authority, as outlined by a formulary in
the Official Journal of the Federation (the official government publication similar to a newspaper or gazette in other countries).
TABLE 9
Nurses’ Prescriptive, Diagnostic, and Referral Authority in Mexico
Nurse Type Prescriptive Authority Diagnosis Referral to Other Services
Auxiliary nurse No No No
Doctoral nurse Yes No No
General nurse/nurse technician No Yes No
Licensed nurse Yes Yes Yes
Master’s nurse Yes No No
Postgraduate nurse Yes Yes Yes
Specialist nurse Yes Ye s Yes
Discipline
Verification of a nursing professional’s credentials and notifications of past or current disciplinary actions are publicly accessible as part
of a nursing registry. In terms of discipline, Mexico commonly uses suspension, revocation, fine or civil penalty, and surrender of license.
South America
Jurisdictions in South America are Argentina, Bolivia, Brazil, Chile, Colombia, Ecuador, Paraguay, Peru, Uruguay, and Venezuela. The
Southern Common Market (MERCOSUR) is a South American regional compact whose member states participate in a common space
to generate business and investment opportunities through the competitive integration of each national economy and the international
market. Regarding nursing, member states are unified by an integrated educational and accreditation framework.
Member states of MERCOSUR include Argentina, Bolivia, Brazil, Paraguay, Uruguay, and Venezuela. Associate members of
MERCOSUR are authorized to participate in meetings regarding common interests within the region and between member states, and
they may enter into economic integration agreements. Associate states include Chile, Colombia, Ecuador, Guyana, Peru, and Suriname.
Guyana and Suriname are included in the section on CARICOM member states, and are not discussed in this section.
Regulation and Governance
Jurisdictions in South America are split as to whether the nursing profession is governed by an independent regulatory body (n = 4) or
a larger agency (n = 5) that also governs other health professions.
The nursing profession in Chile, Colombia, Peru, and Venezuela is governed by independent regulatory bodies. In Chile, Peru,
and Venezuela, each national college of nurses governs the profession. In Colombia, the National Association of Nurses is the regula
-
tory body. Each of these independent bodies holds the power to license or register nurses and regulate for the benefit of public protec-
tion while promoting the nursing profession. Nearly all of these NRBs hold additional powers to discipline nursing professionals and
administer nursing laws and regulations. In Peru and Colombia, each NRB retains the capacity to make decisions about nursing scope
of practice and to handle matters related to the nursing workforce. Chile’s National Association of Nurses holds the power to make
decisions on nursing scope of practice, whereas Venezuela’s College of Nurses holds the power to handle matters related to the nursing
workforce. In Peru, the College of Nurses maintains the broadest powers of the independent regulatory bodies, as it can propose nurs
-
ing legislation, authorize specific certification of nursing practice, handle financial issues related to the profession, and address matters
related to nursing education.
A larger body, such as a Ministry of Public Health, governs nursing in Argentina, Bolivia, Ecuador, Paraguay, and Uruguay. Each
respective body in these jurisdictions regulates nursing and other health professions. These bodies possess the power to license and

36 Journal of Nursing Regulation
discipline nurses, administer nursing laws and regulations, regulate for the benefit of public protection while promoting the nursing
profession, handle matters related to the nursing workforce, and make decisions about nursing scope of practice. Nearly all of these
bodies possess the additional power to create legislation related to nursing. In some instances, the regulatory body can handle matters
of financial and budgetary concern within the profession. The Bolivia Ministry of Health and the Paraguay Ministry of Public Health
and Social Welfare are examples of two bodies that retain such a capacity. Only the Ecuador Ministry of Public Health retains the power
to handle nursing education and training matters.
Nursing in Brazil is governed by both a national regulatory body (the Federal Council of Nurses) and a regional council located in
each of Brazil’s 27 states. These regional councils are independent bodies that solely regulate the nursing profession. Regional nursing
councils follow federal legislation and adhere to state legislation in line with federal law. Each regional council has the power to license,
register, and discipline nurses, promote public protection and the nursing profession, administer nursing laws and regulations, and make
decisions on nursing scope of practice. Most of the regional councils handle nursing workforce and labor matters, as well as budgetary
and financial issues. Notably, regional nursing councils in Rio de Janeiro and Sao Paulo also hold the power to create nursing legislation.
NRB Composition and Members
Many of the governing bodies under a larger agency are comprised of members and representatives who have been nominated and are
then either appointed, elected, or confirmed by the government. Some received their position by ex officio status. Members and repre
-
sentatives are often physicians, nurses, members by ex officio status, or other categories of nursing professionals. Sometimes, such as in
Bolivia’s Ministry of Health, members are comprised of a certain number of public servants. Paraguay’s Ministry of Public Health and
Social Welfare is comprised of 37 representatives. Insufficient data were available as to how many members and representatives serve on
the remaining South American NRBs.
Members are elected in Chile and Peru; in Colombia, some members are elected and others are appointed. There are insufficient
data to determine how Venezuelan members are selected for the NRB.
Each regional nursing council in Brazil consists of the Plenary and the Board of Directors. The Plenary and the Board each retain
a certain number of members proportional to the number of nursing professionals, with additional members as substitutes. Most state
jurisdictions determine the council shall be composed of three-fifths of nurses and two-fifths of other categories of the nursing profes
-
sion, for example, nurse technicians.
In general, regional nursing councils in Brazil are comprised of between five and 21 members who are elected to their positions.
Some regional councils are composed of more members. For example, the Regional Nursing Council of Rio Grande do Sul consists of
27 members, while the Regional Nursing Council of Parana has 36. Every state’s regional nursing council requires council members
to be of Brazilian nationality.
Licensure and Registration Requirements to Practice
Jurisdictions in South America are split almost evenly as to the way they authorize practice for nursing professionals. While all jurisdic-
tions keep a register of nursing professionals, about half use registration alone as a form of authority to practice. Other jurisdictions,
such as Paraguay, Peru, and Uruguay, use a combination of licensing followed by registration. Still other jurisdictions use additional
forms of authorization to practice. In Ecuador, certain nursing professionals, such as advanced practice nurses, nurses, and midwives, are
granted authority to practice by certification and registration, while ancestral midwives are granted authority when they are considered
“legitimized.” Nursing professionals in Argentina are considered authorized to practice after their education is successfully completed.
Each governing regulatory body in Brazil grants authorization to practice by way of registration. Some regional nursing councils
allow a nursing professional to register even if that professional does not yet hold a nursing degree or diploma. If the professional receives
the nursing degree within 12 months of application for registration, the professional is granted authorization.
Qualifying examinations are required for all nurse types in Bolivia, as well as for nurses, midwives, and nursing assistants in Chile.
Nurses and midwives in Ecuador must pass a qualifying examination, as is required of general nurses and midwives in Peru. Argentina
does not require an examination for its nurses or licensed nurses. There are insufficient data to determine whether a national qualifying
examination is required in Brazilian states.
To be considered for authorization to practice, evidence of good moral character is required for most nurse types in all South
American jurisdictions, though these data are lacking for Colombia. For foreign nursing professionals wishing to practice in South
America, some jurisdictions (Argentina, Brazil, Uruguay) require a language proficiency examination. Of the 27 Brazilian states, 23
require foreign nursing professionals to pass a Portuguese language proficiency examination.
Nearly all South American jurisdictions, except for Venezuela, retain a publicly available registry of nursing professionals. This
registry offers individuals and other health professionals the opportunity to verify the authorization status of a nursing professional.
A majority of jurisdictions keep the registry available online, and some make it available within limitations. The Bolivian College of
Nurses makes the registry available, but only within the office of the College of Nurses. As such, an individual may need to request

www.journalofnursingregulation.com 37Volume 10
•
Special Issue
•
January 2020
access to the registry from the College. Similarly, the Ecuador Ministry of Public Health holds the nursing registry within health facili-
ties, health districts, and zones. Likewise, the Paraguay Ministry of Public Health and Social Affairs allows public access to the nursing
registry only after the individual seeking access has applied for a login account.
Following most South American jurisdictions, regional nursing councils in Brazil retain a publicly available registry of nurses.
Some regional councils make theirs available publicly, while most of the regional councils make the registry available online, but by
request of the council. The Regional Nursing Council of Minas Gerais does not make its registry openly available; however, access to
the registry in Minas Gerais may be requested from the Federal Council of Nurses of Brazil.
Nurse Types and Titles
Argentina, Paraguay, and Venezuela recognize the fewest nurse titles. Argentina recognizes a nurse and licensed nurse, where a nurse
holds 3 years of education and a licensed nurse holds 5 years. Paraguay recognizes nurses, nursing assistants, and nursing technicians.
According to available data, Venezuela recognizes the RN role. Chile, Ecuador, Peru, and Uruguay recognize forms of midwife in ad
-
dition to the nurse/RN and nursing assistant/auxiliary nurse roles. Advanced practice or advanced education nurses are recognized in
Bolivia, Chile, Colombia, Ecuador, and Peru. Tables C12 through C15 list the types of nurses among South American jurisdictions and
their entry to nursing requirements.
Nurse types are generally standard across Brazilian jurisdictions. Each state recognizes a nurse, nursing assistant or auxiliary nurse,
and nurse technician. Seventeen Brazilian states recognize either a midwife, an obstetric nurse, or both.
1
Uniquely, Paraiba and Santa
Catarina recognize a nurse specialist or specialist nurse, as Sergipe recognizes a mental health nurse.
Ecuador is unique in that it recognizes not only a midwife specialty, but another type of specialty known as an ancestral midwife
who is a recognized midwife in the community with more than 10 years of experience and who specializes in natural and traditional
Ecuadorean midwifery practices. Ancestral midwives are recognized through a “legitimization” process, which involves midwife training
as well as “community empowerment” training specific to a community or region of the country. An ancestral midwife may also be a
certified midwife who has trained as an ancestral midwife.
Education
Of all the governing regulatory bodies in the South American jurisdictions, the College of Nurses of Peru and the College of Nursing
Professionals of Venezuela hold exclusive authority to approve nursing education and training programs. In other jurisdictions, nursing
education and training programs are either approved by a separate governing body, such as the Ministry of Education, or in cooperation
between the regulatory body of nursing and a separate governing body. For example, the Ministry of Education approves nurse training
and education programs in Brazil. In Bolivia, the Ministry of Health works in cooperation with the Bolivia National Council of Higher
Education and the Bolivia Ministry of Education to approve programs. Similarly, each respective Ministry of Education works in con
-
junction with the NRB in Chile, Ecuador, Paraguay, and Uruguay. In Colombia, a separate College of Association of Nursing Faculty
to approve programs (Tables C12 through C15).
Brazil is a member state of MERCOSUR, so nurse training and education is in line with other MERCOSUR member states—
adhering to an integrated educational and accreditation framework. This is unlike associate member states, where following specific
MERCOSUR education and accreditation framework is not mandatory unless other agreements have been made. MERCOSUR member
states in South America offer bachelor’s degree programs (generally 8 semesters) or 5-year programs for RNs, licensed nurses, and nurses.
MERCOCUR associate members also require university degrees of between six to eight semesters of education and training.
Programs for nursing assistants or nursing technician vary. For example, a program for nursing assistant in Uruguay (a MERCOSUR
member) lasts 24 months, whereas a nursing assistant in Bolivia (Associate MERCOSUR member) lasts 6 months.
In Brazil, regional nursing councils require nurse training and education to be 3-year programs, whereas nursing assistants complete
a program after 1.5 years and nursing technicians complete a diploma or certificate program. Advanced and specialized nurses complete
additional training in their respective specialties after completing initial training as a nurse. Other MERCOSUR member states require
a similar program in nursing that results in a bachelor’s degree or advanced degree in nursing. Brazil’s regional educational program
requirements are shown in Table C16.
Continuing Competence
South American jurisdictions overall require some sort of continuing competence, though data are lacking in terms of the details of this
process for most jurisdictions and nurse types. General nurses and nurse specialists in Peru must complete additional nurse training of
85 hours per year. Uruguay requires participation in professional training and improvement programs for its nursing assistants, RNs,
and midwives, and Venezuela similarly mandates RNs complete “necessary courses for further training and professional development.”
1
Acre, Alagoas, Amazonas, Goias, Mato Grosso, Mato Grosso do Sul, Minas Gerais, Paraiba, Pernambuco, Rio de Janeiro, Rio Grande do Norte, Rio
Grande do Sul, Roraima, Santa Catarina, Sao Paolo, Sergipe, and Tocantins.

38 Journal of Nursing Regulation
Ancestral midwives in Ecuador must go through the legitimization process every 5 years, in a process based on their continued skillset,
knowledge, community and cultural acceptance, and cooperation. Areas of the skillset are sexual and reproductive health, referrals of
pregnant women, care of newborns, obstetric complications, risk situations, and nutrition, among others.
The Brazilian states of Rio de Janeiro, Rio Grande do Sul, and São Paulo do not require continuing competence for their nurses,
nursing assistants, nursing technicians, or midwives. São Paulo also does not require continuing competency for obstetric nurses.
Practice
Although there is limited availability of data within the nursing profession across South America, authorized practice seems to vary
depending on nurse type. In Argentina, nurses and licensed nurses both have prescriptive authority and may prescribe any medica
-
tions. However, neither may refer patients for additional care, nor may they diagnose patients. In Peru, a nurse has a duty to administer
healthcare in an emergent situation and, because of this, nurse specialists and general nurses may prescribe medication or refer patients
for additional medical care. Both nurse types may diagnose patients. Ancestral midwives in Ecuador may refer patients for additional
medical care, diagnose patients, and prescribe medicinal plants and natural remedies.
In Brazil, nurses and advanced or specialized nurses possess authority to offer a nursing diagnosis. In addition, these types of nurses
may prescribe medications according to protocols, clinical and therapeutic guidelines, or other technical regulations established by the
federal, state, or municipal authorities. These protocols and guidelines are subject to the legal provisions of the profession. Prescriptive
authority granted to nurses and advanced or specialized nurses is regarding medications previously established in each respective public
health program and those routinely approved by each health institution. Nurses and advanced or specialized nurses, however, do not have
the autonomy to request examinations and prescribe medications in isolated private practices. These types of nurses must be working
within a health team in order to prescribe, diagnose, or refer and request examinations.
Discipline
South American jurisdictions hold authority to take disciplinary measures against nursing professionals when necessary. Most regulatory
bodies can suspend, revoke, deny, or cancel licenses or authorization to practice. A majority of jurisdictions issue warnings, reprimands,
and fines or civil penalties. Some jurisdictions, such as several Brazilian states and Colombia, issue censures. Peru issues fines and sanc
-
tions, and Peru and Uruguay practice license suspension, denial, and revocation. According to available data, Bolivia may sanction
nurses via registration denial.
Disciplinary measures among the regional nursing councils in Brazil are generally uniform, including censures, suspension, warn
-
ings, fines, cancellation of registration, denial of license, and forms of suspension. As examples of unique sanctions, Paraguay issues a
sanction known as a “call for attention,” while Venezuela issues a sanction depriving honors, rights, and privileges of the professional.
Disciplinary records are available to the public in Colombia, Paraguay, and Brazil. In Colombia, disciplinary records are held and
available at the archives of the Department of Ethical Nursing Tribunals and the National Ethical Nursing Court. In Paraguay, such
records are kept in the same database as the nursing registry. A majority of regional nursing councils in Brazil hold disciplinary records
publicly available, either online or upon an online requesting portal. The Brazilian state of Rio de Janeiro does not allow outright access
to disciplinary records, and similarly, disciplinary records are inaccessible outside of the nursing council in Rio Grande do Sul.
The United States of America
The United States is made up of 50 states, the District of Columbia (or Washington, DC), and five U.S. territories: American Samoa,
Guam, Northern Mariana Islands, Puerto Rico, and the U.S. Virgin Islands (Table 10). Each jurisdiction within the US has its own set
of nursing laws and regulations as well as its own nursing regulatory body or bodies.
The majority of US states are members of the Nurse Licensure Compact (NLC), a mutual recognition compact that allows RNs
and licensed practical nurses (LPNs) to practice in other member states without having to obtain additional licensure. Nurses must
still obtain individual additional licenses to be authorized to practice in jurisdictions that are not members of the NLC. Member states
include Alabama; Arizona; Arkansas; Colorado; Delaware; Florida; Georgia; Idaho; Indiana; Iowa; Kansas; Kentucky; Louisiana; Maine;
Maryland; Mississippi; Missouri; Montana; Nebraska; New Hampshire; New Jersey; New Mexico; North Carolina; North Dakota;
Oklahoma; South Carolina; South Dakota; Tennessee; Texas; Utah; Virginia; West Virginia; Wisconsin; and Wyoming.
Regulation and Governance
There are 60 NRBs (referred to as boards of nursing [BONs]) in the United States. Four states have more than one governing body.
California has the California Board of Registered Nursing and the California Board of Vocational Nursing and Psychiatric Technicians.
Likewise, Louisiana has two nursing regulatory bodies: the Louisiana State Board of Nursing and the Louisiana State Board of Practical
Nurse Examiners. Nebraska has both the Nebraska Board of Nursing and the Nebraska Advanced Practice Registered Nurse Board.

www.journalofnursingregulation.com 39Volume 10
•
Special Issue
•
January 2020
West Virginia has the West Virginia State Board of Examiners for Registered Professional Nurses and the West Virginia State Board of
Examiners for Licensed Practical Nurses.
The mandate, or mission, of the U.S. NRBs is unanimously public protection. All the U.S. NRBs hold the power to regulate for
public protection, administer nursing laws and regulations, license and discipline nursing professionals, and make decisions pertaining
to professional scope of practice. Additionally, many introduce and/or support legislative bills in their state. Almost every governing
body also reserves the authority to approve nursing education programs; however, in three jurisdictions, the authority does not necessarily
lie, at least entirely, with the NRB. Mississippi reserves this authority for the Institutions of Higher Learning, which is the government
body that oversees public education in the state. In New York, this authority belongs to the Professional Education Program Review
unit in the Office of the Professions. Utah relies on U.S. Department of Education–approved national accrediting bodies to oversee
programs, as the statute requires “graduation from an accredited program.” Information on nursing education program approval is not
available for American Samoa or Guam.
The regulatory bodies in most states are composed of a combination of nurses and public members. Nebraska’s, New York’s, and
Puerto Rico’s NRBs are composed entirely of nurses. Nebraska’s advanced practice board, both of Louisiana’s nursing boards, Mississippi’s
board, and both of West Virginia’s nursing boards include nurses, public members, and physicians. Massachusetts is unique in that it
includes nurses, physicians, and at least one pharmacist on its board. Both New Hampshire and Oregon include nursing assistant rep
-
resentatives. Pennsylvania includes the commissioner of the bureau and a licensed dietitian nutritionist, and Utah’s nursing regulatory
body includes the bureau manager. The Northern Mariana Islands’ board is composed of nurses, public members, and either a certified
technician or a certified nursing assistant. The compositions of the American Samoa and Guam NRBs are not publicly available. The
number of members of each U.S. jurisdiction’s NRB is presented in Table 10.
TABLE 10
Number of Members on Nursing Regulatory Bodies in the United States and Its Territories
Jurisdiction Number of Members
States
Alabama Not available
Alaska 7
Arizona 11
Arkansas 13
California—California Board of Regis
-
tered Nursing
6
California—California Board of Vocation
-
al Nursing and Psychiatric Technicians
11
Colorado 11
Connecticut 12
Delaware 15
Florida 13
Georgia 13
Hawaii 9
Idaho 9
Illinois 13
Indiana 9
Iowa 7
Kansas 11
Kentucky 16
Louisiana—Louisiana State Board of
Nursing
11
Louisiana—Louisiana State Board of
Practical Nurse Examiners
12
Maine 9
Maryland 14
Massachusetts 17
Michigan 24
Minnesota 16
Mississippi 13
Jurisdiction Number of Members
Missouri 9
Montana 6
Nebraska—Nebraska Board of Nursing 16
Nebraska—Nebraska Advanced Practice
Registered Nurse Board
9
Nevada 7
New Hampshire 11
New Jersey 15
New Mexico 7
New York 14
North Carolina 14
North Dakota 9
Ohio 13
Oklahoma 11
Oregon 9
Pennsylvania 13
Rhode Island 15
South Carolina 11
South Dakota 11
Tennessee 11
Texas 13
Utah 11
Vermont 11
Virginia 14
Washington 15
West Virginia—West Virginia Board of
Examiners for Registered Professional
Nurses
7
West Virginia—West Virginia State Board
of Examiners for Licensed Practical
Nurses
8

40 Journal of Nursing Regulation
Jurisdiction Number of Members
Wisconsin 9
Wyoming 7
District
District of Columbia (Washington, DC) 11
Territories
2
U.S. nursing diagnoses are based on terminology from the North American Nursing Diagnosis Association.
Jurisdiction Number of Members
American Samoa Not available
Guam 7
Northern Mariana Island 7
Puerto Rico 7
U.S. Virgin Islands 9
Licensure and Registration Requirements to Practice
U.S. jurisdictions license and register LPNs/LVNs and RNs once they have completed their mandatory educational requirements, met
other jurisdiction-specific requirements, and passed a national examination, which is the NCLEX-RN or NCLEX-PN.
All U.S. jurisdictions issue licenses to nurses who are authorized to practice. Licensure information data are stored online at a cen
-
tral database in each state and collectively housed in a national database, Nursys. This information is publicly available on Nursys.com.
APRNs must complete the required education, meet jurisdiction-specific requirements, and pass a national certification examina
-
tion in the population they were educated in. These populations are adult/gerontology (acute or primary care), family, pediatrics (acute
or primary care), women’s health, neonatal, and psychiatric/mental health.
Nurse Types and Titles
There are six types of nurses licensed in the United States (Table C17). Although many practical nurses and RNs specialize in an area,
such as pediatrics or obstetrics, all LPNs/licensed vocational nurses (LVNs) and RNs have a general license. Advanced practice regis
-
tered nurses (APRNs) are licensed, certified, or registered depending on the jurisdiction. The four types of APRNs are certified nurse
practitioner (CNP), clinical nurse specialist, certified nurse anesthetist, and certified nurse midwife. These nurses all have advanced
graduate education beyond that of the RN.
Education
Across all US jurisdictions, LPNs/LVNs nurse programs in the US are generally one to 2 years in duration (Table C17). For RNs in the
US, the duration of education varies. Across all US jurisdictions, RNs may complete either a hospital-affiliated diploma education pro
-
gram, an associate degree program, or a bachelor of science in nursing program in order to qualify to take the NCLEX-RN examination
and become authorized to practice. While the bachelor degree programs are typically 4 years in length, the diploma or associate degree
nursing education programs may be completed in as few as 2 years.
The four APRN roles (CNP, clinical nurse specialist, certified registered nurse anesthetist, and certified nurse midwife) all require
completion of a 2-year masters degree program throughout the US.
Continuing Competence
Most U.S. jurisdictions require evidence of continuing competence for all nurse types, but there are exceptions. Colorado, Guam,
Kentucky, Maine, Mississippi, Missouri, New Hampshire, and New York do not require continuing competence for any of their nurses.
Wisconsin has requirements only for RNs. Connecticut, Louisiana, and Indiana have requirements only for their APRNs. Hawaii, on
the other hand, requires only RNs and LPNs to complete continuing education requirements, leaving APRNs exempt. Continuing
competency requirements are not known for American Samoa.
Practice
In terms of practice, APRNs hold the broadest authority to practice. While authorization varies by each state, APRNs diagnose patients,
refer patients for additional medical treatments/examinations, and have prescriptive authority. CRNAs administer anesthesia.
While RNs may use nursing diagnoses, these are separate and different from the medical diagnoses.
2
RNs in Tennessee have
limited prescriptive authority for oral contraceptives and sexually transmitted disease medications under certain circumstances in gov
-
ernmental settings.
Discipline
In terms of discipline, the following actions are commonly taken by U.S. NRBs: (a) cease and desist orders, (b) reprimand, (c) censure,
(d) summary suspension and suspension, (e) revocation, (f) fine or civil penalties, (g) practice limitation with and without probation, (h)
probation and conditional probation, (i) surrender or denial of license, (j) remediation, (k) assessment of costs, (l) warnings, (m) citation
orders, (n) community service, (o) stipulation to information disposition, (p) voluntary entrance into substance abuse programs, and
(q) other injunctive measures as allowed.

www.journalofnursingregulation.com 41Volume 10
•
Special Issue
•
January 2020
Asia
A
s the largest continent by both land and population, Asia covers an expansive part of the globe. In this report, Asia is grouped
as follows: (a) China and East Asia, (b) Central Asia and India, and (c) Southeast Asia.
China and East Asia
East Asia includes China (People’s Republic of China), Hong Kong (Hong Kong Special Administrative Region of the People’s Republic
of China), Macau (Macao Special Administrative Region of the People’s Republic of China), Japan, Mongolia, North Korea (Democratic
People’s Republic of Korea), South Korea (Republic of Korea), and Taiwan (Republic of China). At the time of publication, informa
-
tion on nursing regulation in North Korea could not be obtained; therefore, it is not included in this profile. This report includes the
remaining countries, which are not members of any regional compacts or mutual agreements that influence the nursing profession.
Regulation and Governance
China, Hong Kong, and Taiwan defer to independent, dedicated nursing councils, while nurses in Japan and South Korea are governed
by their respective Ministry of Health organizations. The multidisciplinary Macau Health Bureau regulates nursing in that Special
Administrative Region of China. Although there are laws related to the regulation of nurses within its Ministry of Health, Mongolia
reports that it does not have a dedicated NRB.
The responsibilities of the regulatory bodies in regions include the authority to require a national examination to practice; simi
-
larly, most regulatory bodies maintain the authority to approve nursing schools or programs, including Hong Kong, Japan, and South
Korea. China, Mongolia, and Taiwan all reserve such authority to their Ministry of Education organizations. The Macau Health Bureau
and the Tertiary Education Services Office of Macau work together to approve nursing education programs.
NRB Mandates
The NRB mandates vary between East Asian countries. China’s, Taiwan’s, South Korea’s, and Japan’s NRBs are charged with protect-
ing the public, promoting the nursing profession, and addressing workforce, labor, or union issues. Macau cites public protection as its
mandate. Hong Kong’s responsibility, on the other hand, is “to fulfill the statutory obligations as stipulated in the Nurses Registration
Ordinance and to ensure the quality of nursing practice in Hong Kong, meeting the rapidly changing healthcare needs of the society
through the establishment of a registration system, provision of guidance, and intervention with discipline.”
3
There are nursing laws in
Mongolia; however, information about the role of the Mongolian Ministry of Health in nursing regulation is not available.
The Chinese Nursing Association is responsible for administrating nursing laws and regulations, licensing and registration, mak
-
ing decisions about scope of practice, and creating legislation. Japan’s Ministry of Health, Labor and Welfare Nursing Policy Division,
the Macau Health Bureau, and Taiwan’s Department of Nursing and Health Care are responsible for each of the above items, but they
also add disciplining nurses to this list. South Korea’s Ministry of Health and Welfare is responsible for each of the items identified by
the Chinese Nursing Association, but they also include disciplining nurses, budgetary matters, and research. The Nursing Council of
Hong Kong has a set of four main functions: (a) “to be responsible for the registration or enrolment of any person qualified in any branch
of nursing and desiring such registration or enrolment;” (b) “to recognize courses of nursing training for the purpose of registration or
enrolment under the [Nurses Registration] Ordinance;” (c) “to determine standards of Licensing Examinations for all branches of nursing
3
National Council of State Boards of Nursing. (2020). Hong Kong. In The Global Regulatory Atlas. https://www.regulatoryatlas.com/jurisdiction-
detail?Jurisdiction=HongKong

42 Journal of Nursing Regulation
under the Ordinance and to be responsible for the conduct of such examinations;” and (d) “to exercise the regulatory and disciplinary
powers for the profession under the Ordinance.”
4
Composition of NRB
The Chinese Nursing Association is composed of members of the China Association for Science and Technology and the Ministry of
Health of China. The Nursing Council of Hong Kong includes the head of nursing service in the Department of Health, six elected
nurses, two appointed members from tertiary institutions that have nursing programs, and one appointed member who falls under the
Hospital Authority Ordinance. Interestingly, one of the nurse members must be a mental disease specialist.
The Macau Health Bureau’s four directors are nominated by the profession and confirmed by the government. Japan’s Ministry
of Health, Labor and Welfare Nursing Policy Division is made up entirely of nurses, and South Korea’s Ministry of Health and Welfare
includes public members as well as a combination of appointed and elected ex officio healthcare personnel. Finally, Taiwan’s Department
of Nursing and Health Care is composed of nurses, public officers, and consultants.
Of the China and East Asia countries that provided NRB information, the following information is available regarding membership
requirements. China requires that council members (a) adhere to the Communist Party’s line, principles, policies, and political quality;
(b) be senior care experts in the nursing discipline; (c) impact the business areas of the Chinese Nursing Association; (d) meet certain age
requirements; (e) be of good health and adhere to a normal working environment; (f) possess full civil capacity; (g) have not been deprived
of political rights for criminal penalties; (h) made outstanding contributions during their Chinese nursing career; and (i) be of high
moral character. Japan requires that members are qualified nurses, midwifes, or public health nurses, while Taiwan merely states there
are “qualification requirements for public service with nursing and healthcare backgrounds.” Requirements are not available for Hong
Kong, Macau, Mongolia, or South Korea. The number of NRB members in the China and East Asia jurisdictions is listed in Table 11.
TABLE 11
Number of Members on Nursing Regulatory Bodies in China and East Asia
4
National Council of State Boards of Nursing. (2020). Hong Kong. In The Global Regulatory Atlas. https://www.regulatoryatlas.com/jurisdiction-
detail?Jurisdiction=Hong%20Kong
Jurisdiction Number of Members
South Korea 95
Taiwan 61
Japan 22
Hong Kong 15
Jurisdiction Number of Members
Macau 4
China Not Available
Mongolia Not Available
Licensure and Registration Requirements to Practice
The Chinese Nursing Association is responsible for licensing and registering nurses. East Asia recognizes nursing professionals as au-
thorized to practice when they have completed their mandatory education and other requirements, including a national examination.
In China, Japan, Macau, Mongolia, South Korea, and Taiwan, a nurse qualification examination is required, while in Hong Kong, only
applicants trained outside of Hong Kong are required to take the national examination—the Licensing Examination for Registration. Taiwan,
Japan, Macau, Mongolia, and South Korea issue licenses to authorized nursing professionals. China requires its nursing professionals to
be registered, and Hong Kong mandates registration and the receipt of a practice certificate.
Once licensed or registered, a public database is typically the means by which a nursing professional’s credentials are verifiable.
China, Hong Kong, Macau, Mongolia, and Taiwan use an online public database. South Korea restricts all nursing-related information
to medical personnel only. Japan presently does not maintain an online database.
Nurse Types and Titles
There are generally four nurse types overall per country, including that of nurse, specialized nurse, midwife, and nurse assistant (Table
C18). China incorporates educational levels into its nurse titles. Macau specifies six different nurse types.
Education
Table C18 lists the educational requirements to become a nurse in China and East Asia.
Continuing Competence
China and Taiwan require continuing education, but the specifics, such as what the requirements are or how often they need to be met,
could not be obtained for this report. China has continuing education requirements in place for nurses and midwives but not for technical

www.journalofnursingregulation.com 43Volume 10
•
Special Issue
•
January 2020
nurses, bachelor’s degree nurses, master’s nurses, doctoral nurses, or associate nurses. Taiwan requires continuing education for each type
of nurse. Hong Kong states that nurses must submit proof of their practicing certificate or license if this credential was awarded by an
authority outside of Hong Kong. Macau states that it requires continuous training of all its nurse types on an annual basis. South Korea
encourages nurses to seek out lifelong education opportunities. Neither Japan nor Mongolia have continuing competence requirements.
Practice
Publicly available practice data for nurses across East Asia are limited. However, nurses are not authorized to prescribe medications, di-
agnose illnesses, or refer patients in China, Hong Kong, South Korea, or Taiwan. Specialty nurses in South Korea can prescribe in certain
emergencies and can diagnose depending on specialty area. Similarly, NPs in Taiwan are authorized to refer patients, but they cannot
prescribe or diagnose. Although nurses in Japan may not prescribe medications or diagnose illnesses, they may refer patients. Nurses in
Mongolia may diagnose but are prohibited from referring patients or prescribing medications. Macau permits nurse specialists, gradu
-
ate nurse specialists, head nurses, and nurse supervisors to refer patients. Grade I nurses may not diagnose or refer patients in Macau.
Discipline
While many countries incorporate a nursing professional’s disciplinary history into their nursing registry, many East Asian countries
do not. Only Hong Kong and Macau make such information publicly accessible. It is not clear what position Mongolia or South Korea
take. In terms of discipline, the following actions are commonly taken in East Asia: (a) reprimand, (b) assessment of costs, (c) removal
of name from registry, (d) suspension, (e) revocation, (f) fine or civil penalty, (g) surrender/denial of license, (h) cease and desist order, (i)
imprisonment, (j) warnings, and (k) practice limitations.
Central Asia and India
Central Asia includes Afghanistan, Bangladesh, Bhutan, Kazakhstan, Kyrgyzstan, Maldives, Nepal, Pakistan, Sri Lanka, and Uzbekistan.
Sufficient data could not be found on Turkmenistan or Tajikistan.
India is comprised of 28 states and nine union territories.
5
Several of these states share mutuality in nursing governance with other
Indian states or territories, namely Andhra Pradesh and Telangana; Assam and Nagaland; Gujarat, Dadra and Nagar Haveli, and Daman
and Diu; Punjab and Chandigarh; Tamil Nadu, Puducherry, and Andaman and Nicobar Islands; and West Bengal and Sikkim. At the
time of this analysis, Dadra and Nagar Haveli, existed as a separate territory from Daman and Diu; on January 26, 2020, these territo
-
ries were combined into a single territory. This analysis reflects the state of nursing regulation in these territories prior to their union.
Regulation and Governance
The nursing profession in Central Asia is primarily governed by larger agency bodies, including Afghanistan, Bhutan, Kazakhstan,
Kyrgyzstan, Sri Lanka, and Uzbekistan. In these countries, nursing governance falls under the authority of each respective Ministry
of Health or a body under the umbrella of the Ministry of Health. In Bhutan, this body is the Bhutan Medical and Health Council.
Similarly, in Sri Lanka, this body is the Medical Council with a division devoted to nursing. In Kazakhstan, Kyrgyzstan, and Uzbekistan,
it is the Ministry of Public Health. Nursing is governed by an independent body in Bangladesh, India, Maldives, Pakistan, and Nepal.
Governing bodies in these jurisdictions consist of a nursing/midwifery council.
In India, a national independent governing body, the Indian Nursing Council, works in cooperation with each independent state
nursing council. A national nursing act sets baseline standards for the nursing profession, and in many states, state nursing acts mirror
the national act and regulate to local state standards. The Indian Nursing Council maintains a national registry database.
Except for Kazakhstan and Sri Lanka, these governing bodies also approve nurse training and education programs. In Kazakhstan,
the Ministry of Education and local regional governments authorize nurse training programs. In Sri Lanka, the nursing council division
of the Medical Council advises the government on matters relating to the education of nursing professionals but does not have exclusive
authority.
State nursing councils generally hold the power to approve nursing education programs, often in conjunction with the Indian
Nursing Council. In Madhya Pradesh, a doctorate or medical education board approves programs. In Mizoram and Tripura, the central
government reserves authority to approve programs. It is unclear as to which governing body holds authority to approve nurse training
and education programs in Uttar Pradesh.
In general, Central Asian NRBs hold the responsibility to license/register and discipline nursing professionals. In addition, they
can regulate for purposes of public protection and the promotion of the nursing profession and administer nursing laws and regulations.
5
A state is a division under Indian constituency, which has a separate government and frames its own laws. Union Territories are ruled directly by the
central government. They are administrated by a lieutenant governor, who represents the president of India and is appointed by the central govern-
ment. See Goswami, K. (2019, August 6). What is the difference between a state and a union territory? India Today. https://www.indiatoday.in/
education-today/gk-current-affairs/story/what-is-the-difference-between-a-state-and-an-union-territory-1577445-2019-08-05

44 Journal of Nursing Regulation
Notably, governing bodies in Bhutan, Kazakhstan, Kyrgyzstan, Nepal, and Pakistan may also create legislation regarding the nursing
profession. The Bangladesh Nursing and Midwifery Council handles nursing work and labor-related issues. The Ministry of Health of
the Kyrgyzstan Republic retains the broadest powers in nursing governance. It holds all the responsibilities mentioned above, in addi
-
tion to the authority to budget and handle financial matters.
Overall, each Indian state nursing council holds the authority to register/license and discipline nursing professionals. State councils
also hold the power to administer nursing laws and regulations and regulate for the purpose of public protection. Nursing councils in
Bihar, Delhi, and Madhya Pradesh hold additional authority to create nursing legislation.
Nearly all jurisdictions in this region have a mandate for public protection. The exceptions are Maldives—where the Nursing
and Midwifery Council reports to the Ministry of Health—and Pakistan, where the nursing council, which reports to the Ministry of
National Health Services. Both nations states that the sole mission of their regulatory bodies is the promotion of the nursing profession.
Promotion of the nursing profession is an additional mission of 28 other jurisdictions in the region, including Afghanistan, Bangladesh
and the majority (n = 26) of the Indian states and territories (excluded are Himachal Pradesh, Kerala, Madhya Pradesh, Meghalaya,
Mizoram, Rajasthan, Sikkim, Tripura, and West Bengal). Delhi (India), Afghanistan, Bangladesh, and Kyrgyzstan also state that mat
-
ters related to the nursing workforce and labor are included in their missions.
NRB Composition
Regulatory bodies throughout Central Asia vary widely in size. Manipur Nursing Council is the smallest with two official members,
whereas Uzbekistan, which regulates nursing through its multidisciplinary Ministry of Health, is the largest with 88 members.
6
The
number of members serving on each NRB is shown in Table 12.
TABLE 12
Number of Members on Nursing Regulatory Bodies in Central Asia and India
6
The Manipur Nursing Council website identifies only two official members of the council: the president and the registrar. According to the Mani-
pur Nursing Council Acts of 2005 and 2008, however, additional members may sit on the council. See Manipur Nursing Council. (2020). http://
www.manipurnursingcouncil.co.in/
Jurisdiction Number of Members
Manipur
a
2
Odisha
a
8
Kyrgyzstan 9
Maldives 9
Chandigarh
b
13
Himachal Pradesh
a
13
Punjab
a
13
Tripura
a
13
Meghalaya
a
14
Mizoram
a
14
Uttar Pradesh
a
14
Delhi
b
15
Haryana
a
15
Goa
a
16
Sikkim
a
17
West Bengal
a
17
Andaman and Nicobar Islands
b
18
Bihar
a
18
Chhattisgarh
a
18
Madhya Pradesh
a
18
Puducherry
b
18
Tamil Nadu
b
18
Jammu and Kashmir
b
19
Jurisdiction Number of Members
Rajasthan
a
20
Dadra and Nagar Haveli
b
21
Daman and Diu
b
21
Gujarat
a
21
Karnataka
a
21
Kerala
a
21
Bangladesh 22
Andhra Pradesh
a
27
Pakistan 31
Kazakhstan 70
Uzbekistan 88
Afghanistan Not data available
Arunachal Pradesh
a
Not available
Assam
a
Not available
Bhutan Not available
Jharkhand
a
Not available
Nagaland
a
Not available
Nepal Not available
Sri Lanka Not available
Telangana
a
Not available
Uttarakhand
a
Not available
Maharashtra Not data available
a
Indian state.
b
Indian territory.

www.journalofnursingregulation.com 45Volume 10
•
Special Issue
•
January 2020
Most (37) of the regulatory bodies in Central Asia include nurses on their regulatory bodies. Seventeen of these regulatory bodies
(13 Indian states plus Afghanistan, Bhutan, Maldives, and Pakistan) also include physicians, and eight regulatory bodies (six Indian
states, Sri Lanka, and Pakistan) include members of the public. Afghanistan includes midwives on its Afghanistan Midwifery and
Nursing Council, which is under the Ministry of Public Health. Kazakhstan reports its Ministry of Healthcare Committee of Public
Health Protection is comprised of physicians and members of the public. Kyrgyzstan also includes healthcare workers and members
of the public in its Ministry of Health but did not specify the professions of its healthcare worker members—Maldives similarly did
not specify the professions of the health care professionals on its Nursing and Midwifery Council, but also specified a lawyer among its
members. Uzbekistan’s Ministry of Health is comprised of public servants who may or may not belong to any specific health profession.
No data were available about the composition of the regulatory body in the Indian states of Arunachal Pradesh, Jharkhand, Telangana,
and Uttarakhand. In Nepal and six of the Indian states, professional associations must be represented on the regulatory body. Nepal, Sri
Lanka, and 11 Indian states include educators on their regulatory body, and eight Indian states specify that high-level nurses from local
hospitals must be included on the regulatory body. Bhutan also ensures that certain specialties are represented.
Many jurisdictions in Central Asia specify eligibility qualifications to serve on the regulatory body. In most cases, the boards dis
-
qualify anyone with a history of insolvency (7 Indian states) or a relevant criminal history (8 Indian states) or specify that the representative
must be of sound mind (6 Indian states). Goa and Nepal require members to have a bachelor’s degree, while Sri Lanka requires certain
members of its regulatory body to have a postgraduate degree. Sri Lanka and Nepal specify that members must have a certain number of
years of nursing practice to serve. Rajasthan declares that noncitizens of India are ineligible, while the states of Haryana and Karnataka
specify any nurse removed from the nursing register is disqualified from serving as a member. Madhya Pradesh mandates that at least
one male nurse serve among the three members of its council elected by RNs. The Indian state of Bihar requires a certain proportion
of its regulatory body to be female, and, interestingly, those serving on the regulatory body in Haryana must be older than 62 years.
Licensure and Registration Requirements to Practice
In general, Central Asian NRBs hold the responsibility to license/register and discipline nursing professionals. In Central Asia and
India, registration is typically the means by which nursing professionals are authorized to practice after having successfully completed
all required education and training. Kyrgyzstan and Uzbekistan are exceptions. In Kyrgyzstan, a nurse specialist must be both licensed
and registered, while other nurse types need only be registered. Similarly, in Uzbekistan, a nurse midwife must be both licensed and
registered, while a midwife is considered authorized to practice after having completed the required education.
In India, apart from Arunachal Pradesh, Madhya Pradesh, Sikkim, and West Bengal, state and territorial jurisdictions also grant
authority to practice to nursing professionals by way of registration. In Arunachal Pradesh, the bachelor of nursing nurse is authorized
by diploma, whereas other nurse types in that state are authorized by registration. In Madhya Pradesh, Sikkim, and West Bengal, nurses
are authorized by both license and registration.
Almost every jurisdiction in Central Asia requires that after successful completion of a nursing program, nursing candidates must
pass a qualifying examination to be considered for practice. The exception is Uzbekistan—no data were found on whether Uzbekistan
requires such an examination. In India, a majority of state and territory jurisdictions require a qualifying examination in order to be
considered for practice for most nurse types. There is typically no qualifying examination for post-basic and specialty nurse type designa
-
tions; however, university examinations or additional qualification in some respect of the training specialty is required.
In Afghanistan, all nurse and midwife types must demonstrate evidence of good moral character and are considered authorized
to practice through registration.
Every Indian jurisdiction and a majority of Central Asian jurisdictions retain a publicly available registry of nursing professionals.
These registries offer individuals and other health professionals the opportunity to verify the authorization status of a nursing professional.
In India, the Indian Nursing Council maintains a national registry bank of nursing professionals. Most states retain their own public
registry either online, published in the state gazette, available at the respective Council office, or by a combination of these methods.
Pakistan, Kazakhstan, Maldives, and Uzbekistan do not offer a publicly available registry of nursing professionals. For the remaining
Central Asian jurisdictions that do, the registry can be found online.
Nurse Types and Titles
Common nurse types across all Central Asian and Indian jurisdictions include general nurses or RNs, midwives, health visitors, nurse-
midwives, auxiliary nurses/nursing assistants, and bachelor’s/basic nurses (Tables C18 through C22). Notably, Bangladesh has six types
of RNs. Pakistan, India, Kyrgyzstan, and Bhutan designate additional nurse types in the area of specialty nurse. For instance, the Bhutan
Medical and Health Council designates a master’s nurse, while the Pakistan Nursing Council designates LPNs, community midwives,
family welfare workers, and lady health visitors. Kyrgyzstan’s Ministry of Health designates seven specialty nurses including obstetric
nurse, nurse anesthetist, nursing nurse, pediatric nurse, physiotherapy nurse, and infectious disease nurse. Afghanistan recognizes an

46 Journal of Nursing Regulation
assistant midwife (who must pass the Afghan National Testing and Certification Midwifery Examination), an auxiliary nurse midwife
(requiring 6 months of training), and a community midwife (requiring 2 years of training).
While India follows both national and state nursing laws, each state is distinct as to which specialty nurse types are designated.
Uttarakhand designates only a few, such as a master’s nurse, health worker, and a post-basic nurse. Maharashtra designates additional
specialty nurses and post-basic nurses, including PhD nurses, master of science in nursing nurses, masters of philosophy in nursing
nurses, psychiatric nurses, pediatric nurses, oncological nurses, and critical care nurses.
Education
Tables C18 through C22 contain the educational requirements to become a nurse in each Central Asian jurisdiction. The Indian nurse
types and requirements are listed as a separate table due to the large number of states and territories involved.
Nursing education in Central Asia and India is consistent for general nurses/RNs and basic nurses. These programs last 3 to 4
years. Nurse training programs for midwives are generally 2 to 3 years.
Central Asian jurisdictions that designate specialty nurse education and training programs are typically an additional 1 to 2 years
following initial training as a nurse or midwife. Some post-basic nursing and PhD programs may be of longer duration.
Continuing Competence
In Central Asia, half of the jurisdictions require some form of continuing competence. Afghanistan does not appear to require any
continuing competence. Data were not available as to whether continuing competence is required in Nepal, Pakistan, Sri Lanka, and
Uzbekistan. The Maldives requires continuing competence on a biennial basis for all 3 of its nurse types: Registered Nurse, Enrolled
Nurse, and Registered Nurse Midwife, which entails educational qualification, good standing, a state examination certificate, and
council registration.
Nearly every Indian state requires some form of continuing education for nursing professionals. No specific data requiring con
-
tinuing competence could be found for Andhra Pradesh and Telangana, Gujarat, Dadra and Naga Haveli, Daman and Diu, Manipur,
and Uttar Pradesh.
Practice
There is limited information regarding areas and scope of authorized practice; Bhutan, Bangladesh, Maldives, and Kazakhstan provide
some information. In Bhutan, both a bachelor’s Nurse and master’s Nurse hold some prescriptive authority. In Bangladesh, an RN
may refer patients for other medical services. In addition, some RN types may diagnose but not on a regular basis. In Kazakhstan, a
bachelor’s degree nurse may make nursing diagnoses and holds prescriptive authority only pertaining to some medications. Midwives
in Afghanistan and Maldives may not prescribe medication.
In India, about half of the state nursing councils articulate extended scope of authority (Table 13). Largely, this includes the
authority to refer patients for other medical care. The Karnataka State Nursing Council allows a registered midwife to also diagnose
pregnancies. Similarly, the Tamil Nadu Nurses and Midwives Council grants a registered nurse midwife prescriptive authority in line
with government standing orders.
TABLE 13
Nursing Scope of Authorized Practice in India
State or Territory Nurse Type Scope of Practice
Andaman and Nicobar Islands (See Tamil Nadu) (See Tamil Nadu)
Chandigarh (See Punjab) (See Punjab)
Chhattisgarh Health visitor May refer patients
Auxiliary nurse midwife May refer patients
General nurse midwife May refer patients
Delhi General nurse midwife May refer patients
Auxiliary nurse May refer patients
Post-basic nurse May refer patients
Haryana Auxiliary nurse Midwife May refer patients when necessary
General nurse Midwife May refer patients when necessary
Jammu and Kashmir Midwife May refer patients
Jharkhand General nurse midwife May refer patients
Manipur General nurse midwife May refer patients
Odisha (formerly Orissa) Midwife May refer patients

www.journalofnursingregulation.com 47Volume 10
•
Special Issue
•
January 2020
TABLE 13 (continued)
State or Territory Nurse Type Scope of Practice
Puducherry (See Tamil Nadu) (See Tamil Nadu)
Punjab Registered nurse May refer patients
Tamil Nadu Registered nurse midwife May refer patients; may prescribe medications per
government standing orders
Uttar Pradesh Midwife May refer patients
General nurse midwife May refer patients
Uttarakhand General nurse midwife May refer patients
Discipline
Nearly all Central Asian jurisdictions hold authority to take disciplinary measures against nursing professionals. Likewise, every Indian
state holds authority to take disciplinary measures against nursing professionals who violate the nursing professional code of ethics. Of the
Central Asian jurisdictions, Pakistan and Kyrgyzstan administer the most forms of disciplinary actions. Afghanistan, Maldives, Pakistan,
Kyrgyzstan, and Uzbekistan implement actions inclusive of license/registration revocation, fines, registration denial, and registration
removal or rejection. Pakistan may also order imprisonment, while Kyrgyzstan may issue a suspension on authority to practice. Bhutan,
Kazakhstan, Nepal, and Sri Lanka may revoke, cancel, or remove a professional’s registration. Additionally, Afghanistan, Nepal, and Sri
Lanka issue fines, with Sri Lanka also retaining the capacity to issue imprisonment as a necessary measure against nursing professionals.
In India, common disciplinary measures include removal, denial, or rejection of registration, fines, warnings, suspensions, and
revocations on authority to practice. Some Indian state and territorial jurisdictions, such as Chhattisgarh, Delhi, Gujarat, Dadra and
Nagar Haveli, Daman and Diu, Haryana, and Jammu and Kashmir sanction by way of imprisonment. The Tamil Nadu Nurses and
Midwives Council implements additional sanctions such as an order to cease and desist, an issue of summary suspension, or a surrender
of authority to practice.
Most jurisdictions in Central Asia and India allow public access to the disciplinary records of nursing professionals. Pakistan,
Kazakhstan, Maldives, and Uzbekistan do not offer a publicly available registry of nursing professionals authorized to practice. For those
that grant access, the records are available online. Nepal also publishes disciplinary records in the national Nepal Gazette. In India, state
and territorial jurisdictions that hold disciplinary records open to the public are Chhattisgarh, Goa, Himachal Pradesh, Jammu and
Kashmir, Kerala, Karnataka, Madhya Pradesh, Maharashtra, Manipur, Meghalaya, Orissa, Sikkim, Tripura, Uttar Pradesh, Uttarakhand,
and West Bengal. These jurisdictions publish records either online, in a gazette or newspaper, or make them available in the respective
state nursing council offices.
Southeast Asia
Southeast Asia includes Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, the Philippines, Singapore, Thailand, Timor-Leste
(formerly East Timor), and Vietnam. Currently, all 10 of these countries belong to the Association of Southeast Asian Nations (ASEAN).
Regulation and Governance
Both independent and larger agency bodies regulate the nursing profession throughout Southeast Asia. Brunei, Cambodia, Myanmar, the
Philippines, Singapore, and Thailand are governed by an independent body, while Indonesia, Laos, Malaysia, Timor-Leste, and Vietnam
defer to their Ministry of Health bodies for nursing governance. The mandate of all Southeast Asian NRBs are public protection and/
or promotion of the profession. Myanmar and Timor-Leste lists workforce, labor, and union issues as an additional mandate, and Timor-
Leste additionally cites education and training as a mandate.
The Indonesia and Malaysia NRBs are comprised of nurses, physicians, and/or health professionals, whereas Laos and Vietnam list
the composition as public servants. Myanmar, the Philippines, and Thailand require that members are nurses. There are no data available
for the remaining Southeast Asian NRBs. The number of members serving on each NRB is shown in Table 14.

48 Journal of Nursing Regulation
TABLE 14
Number of Members on Nursing Regulatory Bodies in Southeast Asia
Country Number of Members
Philippines 7
Brunei 12
Singapore 17
Malaysia 21
Cambodia 32
Country Number of Members
Thailand 32
Myanmar 60
Indonesia Not available
Laos Not available
Timor-Leste Not Available
Vietnam Not available
The authority to require a national examination to practice is granted to most regulatory bodies in the region, with Cambodia
being the lone exception. Additionally, no data is available as to whether the Indonesian Ministry of Health maintains this authority.
Similarly, some regulatory bodies maintain the sole authority to approve nursing schools or programs, including Brunei, Myanmar,
Singapore, and Thailand. Others share such authority with their respective Ministries of Education, Qualification Agencies, or Higher
Education Commissions, including Laos, Malaysia, and the Philippines by other branches of the government: the Ministry of Education
in Vietnam. Information is not publicly available as to whether the Indonesian Ministry of Health maintains the authority to approve
nursing schools or programs.
Additionally, the responsibilities of all the Southeast Asian NRBs include administering nursing laws and regulations, licens
-
ing/registering nurses, and making decisions about scope of practice. Almost all Southeast Asian NRBs except for Indonesia include
disciplining nurses under their powers of governance.
Licensure and Registration Requirements to Practice
Six Southeast Asian countries (Brunei, Cambodia, Laos, Malaysia, Myanmar, and the Philippines) require a national examination for
all nurse types. Singapore and Vietnam do not require a national examination for nurses. Thailand requires an examination for profes
-
sional nurses, NPs, nurse anesthetists, midwives, and nurse specialists. It does not require an examination for nursing assistants and
post-NPs. Timor-Leste requires an exam for Basic Nurses and General Nurses, but its Specialist Nurse requirements vary. There are no
data available for Indonesia.
In Brunei, Cambodia, Malaysia, the Philippines, and Singapore, nursing professionals must be registered in order to practice
nursing, whereas Indonesia, Laos, Thailand, and Vietnam issue licenses to authorized nursing professionals. Registration and licensure
are both required for authorized nursing practice in Myanmar. Timor-Leste requires registration, license, and diploma for all nurse types
except Basic Nursing, which only requires a diploma. Malaysia, Myanmar, and the Philippines require a language proficiency examina
-
tion for nurses from outside their countries.
Once licensed and/or registered, a public database is typically the means by which a nursing professional’s credentials are verifi
-
able. Much of Southeast Asia relies significantly on physical databases, such as a national newspaper or gazette or the internal records of
a respective nursing council office. Only the Philippines and Singapore use an online public database. Brunei, Indonesia, and Thailand
rely on physical means of providing access to their nursing registries. Cambodia and Vietnam restrict public access altogether. There
is no available information as to whether Laos, Malaysia, Myanmar, or Timor-Leste restrict their registry or use a physical database.
Nurse Types and Titles
There are generally three to four nurse types per country, including nurse, midwife, specialized nurse, and nurse assistant (Table C23).
However, some jurisdictions designate specific specialized nurses. Brunei, for instance, recognizes children’s nurses, mental health
nurses, and infectious disease nurses. Additionally, Malaysia recognizes public health nurses and community nurses, and Thailand also
recognizes nurse anesthetists. In addition to nursing assistant and midwife, Timor-Leste recognizes the following categories: basic nurs
-
ing (a bachelor’s degree in nursing), specialist nurse, general nurse, coordinating nurse, and head nurse. It also designates a midwife
and two advanced levels of midwives, contingent on years of experience and/or performance evaluation: professional midwife senior and
professional midwife specialist.
Education
Table C23 shows the requirements for entry into each type of nursing education program within each Southeast Asian jurisdiction. There
are no data available for the duration and program entry requirements for Brunei. The majority of the remaining nursing programs are
between 3 and 4 years in duration.

www.journalofnursingregulation.com 49Volume 10
•
Special Issue
•
January 2020
Continuing Competence
Much of Southeast Asia requires continuing competence, except for Singapore. Data are not available as to whether Indonesia mandates
continuing competence among its national nursing regulations. Cambodia requires 40 hours per year of continuing professional de
-
velopment; Malaysia mandates 25 to 35 credit hours annually; Thailand requires 50 continuing education units every 5 years with the
renewal of the nursing license; and Vietnam mandates 48 hours of continuing education every 2 years. Timor-Leste states that “nurs
-
ing progression is subject to the Technical Commission for the Evolution of Health Professionals (CTEPS),” and that upon renewal of
registration, all nurse types must submit proof of criminal record clearance and documents proving that they are not inhibited from
exercising the profession, have not been expelled from his/her profession, and are complying with any disciplinary sanctions of suspen
-
sion of the exercise of the profession.
7
Practice
Overall, practice information is limited in Southeast Asia. Data related to areas of authorized practice for RNs are unavailable in Brunei,
Indonesia, Malaysia, the Philippines, and Timor-Leste. In Cambodia, all nurses may refer patients; associate and bachelor degree nurses
may also diagnose illnesses. RNs in Laos are restricted from referring patients and diagnosing illnesses, but information related to
their authority to prescribe medication is unavailable. Similarly, RNs and nurse midwives in Myanmar may formulate diagnoses, but
prescribing authority information is unavailable. Although nurses in Singapore also lack the authority to prescribe medications, they
may refer patients. Information on their authority to diagnose illnesses is not available. Professional nurses in Thailand cannot prescribe
medications, refer patients, or diagnose; however, specialized nurses such as NPs are authorized to perform those functions. Midwives
may refer patients in Timor-Leste. Nurses in Vietnam appear to maintain the greatest level of authority as both nurses and midwives
are authorized to prescribe medications, diagnose illnesses, and refer patients.
Discipline
Information related to the availability of disciplinary records is mostly unavailable throughout the entire region with the exceptions of
Myanmar, Timor-Leste, and Thailand. Myanmar public access, whereas Thailand and Timor-Leste grant public access. In terms of dis
-
cipline, the following actions are commonly taken in Southeast Asia: (a) suspension, (b) revocation, (c) fine or civil penalty, (d) surrender
or denial of license, (e) denial or removal of name from register, (f) imprisonment, (g) warnings, (h) practice limitation, (i) probation, (j)
reprimand, (k) censure, and (l) community service.
7
National Council of State Boards of Nursing. (2019). Timor-Leste. In The Global Regulatory Atlas. Unpublished raw data.

50 Journal of Nursing Regulation
Australia and Oceania
O
ceania includes the Cook Islands, Fiji, Kiribati, the Marshall Islands, Micronesia, Nauru, New Zealand, Palau, Papua New
Guinea, Samoa, the Solomon Islands, Tonga, Tuvalu, and Vanuatu. New Zealand and Australia are members of the Trans–
Tasman mutual recognition group. This compact encourages mobility and provides for an individual who is registered in
connection with an occupation in New Zealand to carry on an equivalent occupation in Australia, and vice versa; therefore, enrolled
nurses, registered nurses and nurse practitioners are mutually recognized throughout Australia and New Zealand. Additionally, Nauru
and Australia have an agreement that allows nursing professionals from Australia to treat patients in Nauru without being subject to
registration or licensing requirements under the laws of Nauru.
The Northern Mariana Islands and Guam are also geographically located in this region; however, as U.S. territories, they are
discussed in the United States section.
Regulation and Governance
Independent nursing councils regulate the nursing profession throughout Oceania and Australia, governing approximately two-thirds
of the region, including Australia, the Cook Islands, Fiji, Kiribati, the Marshall Islands, Micronesia, New Zealand, Samoa, the Solomon
Islands, Tonga, and Vanuatu. Larger bodies, commonly the Ministry of Health, govern nursing in the remaining countries of Nauru,
Palau, Papua New Guinea, and Tuvalu.
The NRB mandate in all of Australia and Oceania is public protection. In fact, this is the only mandate in seven countries (Australia,
New Zealand, Papua New Guinea, Samoa, Tonga, Tuvalu, and Vanuatu).
Eight NRBs have additional mandates that include promotion of the nursing profession (Cook Islands, Fiji, Kiribati, Marshall
Islands, Micronesia, Nauru, Palau and the Solomon Islands). Additional mandates of Oceanic NRBs include workforce, labor, and union
issues (Fiji and Nauru); developing administrative procedures and disciplinary measures (the Marshall Islands); and creating, developing,
and amending nursing regulations and standards (Micronesia).
All NRBs in Oceania have the responsibility of administrating nursing laws and regulations, and disciplining nurses. Thirteen
NRBs have the additional responsibility of making decisions about scope of practice (Australia, Cook Islands, Fiji, the Marshall Islands,
Micronesia, Nauru, New Zealand, Palau, Papua New Guinea, Samoa, Tonga, Tuvalu, and Vanuatu). Ten NRBs are also responsible for
matters related to nursing education or training (Cook Islands, Fiji, Kiribati, the Marshall Islands, Micronesia, Nauru, Palau, the Solomon
Islands, Tonga, and Tuvalu). Five NRBs have the additional power to create legislation (Fiji, Papua New Guinea, Samoa, Tonga, and
Vanuatu). Tonga’s NRB has the additional responsibility of advising the minister on nursing matters.
Composition of NRBs
The NRBs in Australia and Oceania are generally composed of nurses, public members, and other health officials. While all NRBs
include nurses, Micronesia is the only jurisdiction whose National Board of Nursing is composed entirely of nurses. Most of the Oceanic
jurisdictions (Australia, Cook Islands, Kiribati, Marshall Islands, Nauru, New Zealand, Palau, Samoa, and Tonga) also include members
of the public on their regulatory bodies. Several jurisdictions (Australia, Fiji, Marshall Islands, Palau, Tuvalu, and Vanuatu) have NRBs
with members of other health professions serving on their nursing regulatory body. Tuvalu, Palau, and Papua New Guinea specify a
physician or medical practitioner must be involved in the regulatory body. Kiribati and Vanuatu also include a lawyer on their regula
-
tory body, and Nauru includes a member of the clergy.
NRB members are appointed by the government in Australia, the Cook Islands, Fiji, Kiribati, Micronesia, Nauru, Papua New
Guinea, Samoa, and Vanuatu. In five countries (the Marshall Islands, New Zealand, Palau, the Solomon Islands, and Tonga), the NRB

www.journalofnursingregulation.com 51Volume 10
•
Special Issue
•
January 2020
members are nominated by the profession and confirmed by the government and/or minister. There is no information on the selection
process for Tuvalu’s NRB members.
Most NRBs in this region require nurses on the NRB to be actively enrolled as a nurse and in practice for 3 to 5 years (Fiji,
Kiribati, Marshall Islands, Micronesia, Papua New Guinea, Samoa, Tonga and Vanuatu). Additionally, in the Marshall Islands and
Palau, the public member on the Board cannot be a member of any health-related profession, cannot have a conflict of interest, and
must have at least a high school diploma or its equivalent. Micronesia also requires that every island in their nation is represented with
a member or members.
In the Solomon Islands, NRB members must not have a mental or physical disability that inhibits the functions of the office
and must display conduct consistent with the office. Five jurisdictions (Australia, the Cook Islands, Nauru, New Zealand, and Tuvalu)
provide no publicly available information related to the competencies or qualifications required to serve on the NRB.
The number of members serving on each NRB is shown in Table 15.
TABLE 15
Number of Members on Nursing Regulatory Bodies in Australia and Oceania
Jurisdiction Number of Members
Micronesia 5
Nauru 5
Cook Islands 6
Kiribati 6
Tonga 6
Tuvalu 6
Marshall Islands 7
Vanuatu 7
Jurisdiction Number of Members
Papua New Guinea 8
New Zealand 9
Palau 9
Samoa 9
Fiji 11
Australia 12
Solomon Islands No data
Licensure and Registration Requirements to Practice
The powers and responsibilities granted to the NRBs in Australia and Oceania are broad and include the responsibility of licensing/
registering nurses, the authority to require a national examination to practice nursing. Most Oceania NRBs require a licensure ex
-
amination (or its equivalent) for their nurse types. The exception is New Zealand, where RNs, enrolled nurses, and NPs must pass an
examination, but there is no required examination for RN prescribers in primary or community health. Apart from the payment of
applicable fees, the only other requirement for authorization to practice among Oceanic jurisdictions is, in the case of Nauru and Palau,
that nurses carry malpractice insurance.
Australia and Oceania recognize authorized nursing professionals who have completed their mandatory education and other re
-
quirements in the granting of nursing licensure and/or registration. Nearly all nursing governing bodies in Australia and Oceania use
registration to authorize at least some nurse roles for practice, but there are a few exceptions. In Papua New Guinea, nearly all nurse
roles must be both licensed and registered. The exception is registered midwives who may practice immediately upon completing their
education. Likewise, Micronesia requires its RNs, LPNs, and advanced practice nurses to be both licensed and registered, while NPs,
nurse midwives, and nurse anesthetists need only register. Additionally, to have the title of “enrolled nurse” in Kiribati, only a diploma
is required, and to be a medical assistant, an additional certificate is needed after registration. Nurse aids in the Solomon Islands must
also obtain both a certificate and registration. In New Zealand, all nurse roles are issued an annual practicing certificate.
Once registered and/or licensed, a public database is typically the means by which a nursing professional’s credentials are verified.
In general, most countries in Oceania do not use an online public database. Instead, they make such information available in physical
form, such as in a newspaper or gazette. Australia and New Zealand are the only two countries in the region that employ an online
system. Micronesia makes its nursing registry available only to employers or other licensing boards outside of Micronesia, but not to
the general public.
Nurse Types and Titles
In addition to nurse, midwife, specialized nurse, and nurse assistant categories, some countries—such as the Marshall Islands—recognize
as many as nine nurse types (Tables C24 through C27).

52 Journal of Nursing Regulation
Education
Australia and Oceania have the authority to approve nursing schools and programs. Tables C24 through C27 show the requirements for
entry into each type of nursing education program within Australia and Oceania.
Continuing Competence
Continuing competence is a requirement in Australia, the Cook Islands, Fiji, the Marshall Islands, Micronesia, New Zealand, Palau, and
Tuvalu, although details were not publicly available as to what specific continuing competence requirements entailed. No information
is available as to what position Kiribati, Nauru, Papua New Guinea, Samoa, the Solomon Islands, Tonga and Vanuatu take concerning
continuing education requirements.
Practice
Publicly available areas of authorized practice data for nurses across Australia and Oceania are limited. For eight NRBs, no information
is publicly available as to what type of authority RNs have across countries (Fiji, Micronesia, Nauru, Samoa, the Solomon Islands, Tonga,
Tuvalu, and Vanuatu). In Australia and New Zealand, RNs can only diagnose illnesses, while NPs may diagnose illnesses, prescribe
medications, and refer patients. Mental health nurses in the Cook Islands may prescribe medications and refer patients in accordance
with Community Treatment Order guidelines.
Discipline
In addition to verifying a nursing professional’s credentials, notifications of past or current disciplinary actions are also publicly acces-
sible as part of a nursing registry. In terms of discipline, the following actions are commonly taken in Australia and Oceania: reprimand,
suspension, fine or civil penalty, revocation, surrender or denial of license, removal or refusal of name from register, imprisonment, license
restriction, and medical or psychological treatment. There is no information available as to whether Fiji, the Marshall Islands, Palau,
Papua New Guinea, or Samoa make their disciplinary records publicly accessible. Most others do so, except New Zealand.

www.journalofnursingregulation.com 53Volume 10
•
Special Issue
•
January 2020
Europe
E
urope encompasses Eastern Europe, the Nordic region, and Western and Central Europe.
Eastern Europe
Eastern Europe is comprised of Albania, Belarus, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Estonia, Greece, Latvia, Lithuania,
North Macedonia (former Yugoslav Republic of Macedonia), Moldova, Montenegro, Romania, Russia, Serbia, Turkey, and Ukraine. Of
those countries, Bulgaria, Croatia, Cyprus, Estonia, Greece, Latvia, Lithuania, and Romania are members of the EU.
Regulation and Governance
Bosnia and Herzegovina, Croatia, Cyprus, Greece, Romania, Serbia, and Ukraine have independent nursing bodies that regulate nurses.
Albania, Belarus, Bulgaria, Estonia, Latvia, Lithuania, North Macedonia, Moldova, Montenegro, Russia, and Turkey have NRBs that
are part of a governing body that regulates many professions. These NRBs are often part of the Ministry of Health.
NRB Mandates
NRBs in Eastern Europe have varying mandates and most include public protection except for Estonia, which is charged with promo-
tion of the profession of nursing and workforce, labor, and union issues. Promotion of the profession is mandated in 11 of the reporting
jurisdictions. Workforce, labor, and unions issues were reported as NRB mandates in Bulgaria, Estonia, Lithuania, North Macedonia,
and Serbia.
Responsibilities of the NRBs vary across this region. Promotion of other health professionals and public protection under the
umbrella of the Bulgarian Association of Health Professionals in Nursing is included in Bulgaria. The NRB in Lithuania is responsible
for policy making in the field of nursing and legal regulation of nursing practice. Romanian NRBs are mandated with jurisdiction
regulation, surveillance of continued professional development, and recognition of quality. In Russia, the Ministry determines entry
requirements to nursing professions, as well as practice in nursing professions and standards and procedures of providing care.
The majority of NRBs are empowered to administer nursing laws and regulations, make decisions about scope of practice, disci
-
pline nurses, and participate in the creation of legislation. The Bulgarian Association of Health Professionals in Nursing also handles
economic matters related to the Association and provides financial and logistical support. Ukraine provides consultation on nursing-
related employment in Ukraine and abroad. Additionally, the Ministry of Education or a related national accrediting agency in most
countries is tasked with the responsibility of approving nursing schools/programs in the majority of nations in this region. Bulgaria,
Latvia, Lithuania, Montenegro, Russia, and Turkey, however, grant such authority to their Ministry of Health organizations. The Nursing
and Midwifery Council of Cyprus is charged with this responsibility.
NRB Composition
NRBs in Croatia, Greece, Lithuania, and Romania are composed of nurses. Albania includes nurses and public members. Nurses, nurs-
ing technicians, health workers, and ex officio members comprise the NRB in Bosnia and Herzegovina. This duty is shared in Bulgaria
by nurses and other regulated health professionals. The NRB in Cyprus is composed of nurses, midwives, and health visitors. Public
officials and ex officios in Belarus serve on NRBs. NRBs in Moldova, Serbia, and Turkey are composed of public servants. The regulatory
body in Montenegro is composed entirely of physicians; in North Macedonia, it includes physicians, public officials, and ex officios. In
Russia, the NRB within the Ministry of Health is composed of civil servants, some of whom have medical education or nurse training.
No members of the Russian Ministry of Health are tasked specifically with regulating nursing. Table 16 includes information from the
10 jurisdictions reporting on qualifications of their respective NRBs.

54 Journal of Nursing Regulation
TABLE 16
Number and Qualifications of Members on Nursing Regulatory Bodies in Eastern Europea
Jurisdiction Number of Members Qualifications to Serve on NRB
Albania 25 No data
Belarus 7 No data
Bosnia and Herzegovina 24 No data on initial qualifications. For representative
renewal, continuous professional training is required
according to the Rules of the Chamber.
Bulgaria 64 The Congress is comprised of the regional college
representatives, who are elected as 1 representative
per every 75 members
Croatia 22 Registered nurse with active license
Cyprus 11 Registration as a nurse or midwife and member of
the Cyprus Nurse/Midwives Association
Greece 15 No data
Latvia 14 representatives right now, but this varies based
on the prime minister (who can appoint a deputy,
ministers for special assignments, etc.)
No data
Romania There are two levels of governance. Level 1 (nation
-
al): Executive Board of 6 members, president, 4 vice
presidents, and secretary. Level 2 (county): 4 mem
-
bers, president, 2 vice presidents, and secretary,
which together compose the National Council.
It is required to be a registered member with a free
right of practice in order to have the right to submit
candidacy.
Russia No data Requirements toward qualifications are based on the
professional position; nursing is not a part of these
requirements.
a
This table includes the 10 jurisdictions in Eastern Europe with available information.
Licensure and Registration Requirements to Practice
The majority of NRBs are empowered to license and register nurses. Eastern Europe recognizes authorized nursing professionals who
have completed their mandatory education and other requirements in the granting of nursing licensure, certification, registration, or
accreditation.
In some jurisdictions, additional requirements beyond education may be necessary prior to authorization to practice nursing.
Romanian nurses are granted registration after completing the program, taking the examination, obtaining malpractice insurance, taking
continuing professional development credits, obtaining medical certification, and providing proof of no criminal record and obtaining
annual authorization if no criminal record is registered. Letters of recommendation are required in Ukraine as evidence of good moral
character. Bulgaria requires certification of no professional offenses, and Cyprus requires a certificate showing no criminal record. Albania
and Belarus also require evidence of good moral character; however, means for this evaluation are not available. Bosnia and Herzegovina
applicants must be dignified, responsible, professional in profession and person, and uphold the ethics of the profession. They must also
submit for licensure a statement and declaration on respecting ethical and deontological principles of profession.
Croatia, Estonia, and Romania do not require a national examination to practice nursing. Examinations are required in Albania,
Belarus, Bosnia and Herzegovina, Bulgaria, Greece, Latvia, North Macedonia, Russia, Serbia, and Ukraine.
A language proficiency examination is required for internationally educated nurses wishing to work in most every Eastern European
jurisdiction except Bulgaria, Croatia, Romania, and Russia. In Russia, although there is no language proficiency examination, the ex
-
amination that grants permission to work is only available in Russian. In Bosnia and Herzegovina there is a possibility of a language
proficiency examination depending on condition of knowledge of the language.
Nurse Types and Titles
Overall, there are generally four nurse types in Eastern Europe, including nurses, midwives, specialized nurses, and nurse assistants.
Denmark has 8 nurse titles. Nurse titles are detailed in Table C28.
Education
Table C28 presents the types of nurses and educational requirements for entry into nursing programs in Eastern Europe.

www.journalofnursingregulation.com 55Volume 10
•
Special Issue
•
January 2020
Continuing Competence
Most of the reporting jurisdictions require continuing education or training. Bulgaria and Greece do not have a requirement of continued
competence for nurses. Russia has the most robust requirements for continued competence of the Eastern European jurisdictions. Every
5 years, all medical professionals are required to receive special training, which includes improvement of qualifications and reexamina
-
tion. A certificate is issued following the examination. This certificate is the document that grants permission to continue practicing in
a nursing role. This system is currently in the process of being reformed. The new procedure will require annual reexamination, as well
as proof of continuing education. In addition, there are requirements regarding state of health such as regular health checks. For those
who practice in pediatric care, applicants must have a lack of criminal record in specific areas.
Bosnia and Herzegovina require annual seminars, courses, expert meetings in nursing and midwifery, and on-the-job training.
Nurses in Estonia must have 60 hours of employer-provided training every year. The NRB in Lithuania requires at least 3 years of legal
nursing practice during the past 5 years and 60 hours of mandatory advanced training during the past 5-year period or 160 hours of
nursing advanced training on or after 5 years. Annual continuing professional development is mandatory in Romania. Serbian nurses
must attain 168 points in order to satisfy continuing education credits—half of the total points must be derived from where the health
professional is employed and the remaining half of the total points are attained via participation in external continuing education pro
-
grams. Ukrainian nurses complete a continuing training requirement every 5 years.
Practice
Authorized nurse practice data is lacking in Europe. The information that is publicly accessible suggests the levels of autonomy can
vary significantly for nursing professionals. For example, nurses and midwives in Albania may prescribe medications, refer patients, and
diagnose illnesses, while nurses and midwives in Ukraine do not have authority to perform those same functions.
Discipline
Discipline is a role of the NRBs in more than half of the countries. Bulgaria, Estonia, Lithuania, Montenegro, Russia, Turkey, and
Ukraine do not have governance over nursing discipline.
The following actions are commonly taken in Eastern Europe: (a) reprimand, (b) suspension, (c) fine or civil penalty, (d) denial
or termination of license, (e) denial or removal of name from register, (f) revocation, (g) censure, (h) probation, (i) warnings, (j) practice
limitation, and (k) cease and desist orders. In addition to verifying a nursing professional’s credentials, notifications of past or current
disciplinary actions are also publicly accessible as part of a nursing registry.
Nordic Region
The Nordic region encompasses Denmark, the Faroe Islands, Finland, Greenland, Iceland, Norway, and Sweden. Of these, Denmark,
Finland, and Sweden are members of the European Union (EU).
Regulation and Governance
Aside from Iceland, NRBs in the Nordic region are part of larger governing agencies such as the Ministry of Health that regulate several
professions. In Iceland, the nursing profession is jointly regulated by the medical director of health, university faculty, and the Icelandic
Nurses Association.
The mandates of the Nordic NRBs are public protection and the promotion of the nursing profession. Denmark and Iceland also
list workforce, labor, or union issues as part of their mandate. The responsibilities and powers of the NRBs in Denmark, the Faroe Islands,
Norway, and Sweden include licensing/registering nurses, administrating nursing laws and regulations, making decisions about scope
of practice, creating legislation, and disciplining nurses. Greenland’s NRB has the additional responsibility of education and training.
Finland’s NRB only focuses on licensing nurses and making decisions about scope of practice. In Iceland, the medical director of health
holds decision-making power jointly with university faculty and the Icelandic Nurses Association, and their only responsibility is li
-
censing/registering nurses. All NRBs in the Nordic region possess the authority to require a national examination to practice nursing;
however, Denmark shares such decision-making power with the Ministry of Education and the National Board of Health.
NRB composition
In Iceland, all members of the NRB are nurses and are appointed by the government. The other Nordic countries’ NRBs are comprised
of a mix of health and education members. In Finland and Sweden, members are required to represent healthcare and educational au
-
thorities, faculties of medicine, and other educational institutions responsible for educating healthcare professionals.
In Finland and Iceland, members serving on the regulatory body are appointed; in Sweden, members take office as public ser
-
vants. In the Faroe Islands, those serving on the regulatory body are nominated by the profession. Denmark’s regulatory body confirms

56 Journal of Nursing Regulation
members through a combination of appointment, nomination, and election. Data were not publicly available as to how Greenland or
Norway choose their members. Table 17 lists the number of members on each NRB.
TABLE 17
Number of Members on Nursing Regulatory Bodies in Europe—Nordic Countries
Country Number of Members
Sweden 8
Faroe Islands 19
Finland 24
Denmark 81
Country Number of Members
Greenland No data
Iceland No data
Norway No data
Licensure and Registration Requirements to Practice
The Nordic region authorizes nursing professionals who have completed their mandatory education and other requirements by grant-
ing a nursing license and/or registration. Overall, registration is required in most Nordic countries except for Iceland, which requires a
nursing license. Finland and Sweden require both registration and licensure.
Denmark, Finland, Greenland, Norway, and Sweden all require passing a licensure examination (or its foreign equivalent) to
become a nurse or midwife. The Faroe Islands has the authority to issue a licensure examination, but information about whether an
examination is required is not publicly available. No examination is currently administered in Iceland, although the regulatory body
has the authority to require one.
Once registered and/or licensed, a public database is typically the means by which a nursing professional’s credentials are verifi
-
able. This may take the form of a physical document, such as a journal, newspaper or gazette stored at the Ministry’s headquarters.
Most commonly, however, this information is available online through the Ministry of Health’s website. Denmark, Finland, the Faroe
Islands, and Norway all maintain an online database of registered nursing professionals that is accessible to the public. Sweden does
not maintain an online database but allows an individual to attain information about a nurse via formal online or mail request. Iceland
does not appear to maintain a public database, while Greenland’s regulatory body provides the public with access to the register in hard
copy, housed at the National Board of Governors and Health headquarters. In addition to verifying a nursing professional’s credentials,
notifications of past or current disciplinary actions are also publicly accessible as part of a nursing registry.
The NRBs of Denmark and Sweden also review criminal backgrounds of potential nurses. No information regarding criminal
background checks was found for other Nordic countries.
Nurse Types and Titles
Aside from Denmark, there are generally two to four nurse types per country, including nurses, midwives, specialized nurses, and nurse
assistants. Denmark has 8 nurse titles (Table 18).
TABLE 18
Nurse Titles in Nordic Countries
Country Nurse Title
Denmark Nurse
Midwife
Psychiatric nurse
Intensive care nurse
Nurse anesthetist
Hygiene nurse
Cancer care nurse
Health visitor
Faroe Islands Nurse
Midwife
Finland Nurse
Midwife
Public health nurse
Country Nurse Title
Greenland Nurse
Midwife
Health assistant
Health worker
Iceland Nurse
Specialist nurse
Norway Midwife
Auxiliary nurse
General nurse
Sweden Nurse
Midwife
District nurse
Specialist nurse

www.journalofnursingregulation.com 57Volume 10
•
Special Issue
•
January 2020
Education
The Nordic regulatory bodies with smaller populations (Iceland, the Faroe Islands, and Greenland) approve nursing schools and pro-
grams. In countries with larger populations (Norway, Sweden, Denmark, and Finland), the authority to approve nursing programs or
schools is reserved for the Ministry of Education.
As seen in Tables C29 through C31, nurses in Nordic countries are generally required to complete secondary school or up to 10
years of general education before they are allowed entry into a nursing program. The length of the nursing programs in the Nordic
region range from 3 to 4 years.
The requirements for entry into a midwifery program vary by each country (Table C35). Sweden requires a complete bachelor’s
degree in a health science, along with 1 year of professional nursing experience. Finland also requires candidates to have completed
their RN program. Denmark only requires the completion of a high school education, and Greenland requires permanent residency in
addition to completion of a secondary school education. Midwifery programs in the Nordic region are between 1 to 3.5 years in length.
Table C36 displays the types of specialty nurses in Denmark, as well as the length of each nursing program and requirements for
entry.
Continuing Competence Requirements
Regarding Continuing Competence , Norway and Denmark encourage lifelong learning in their nurses, whereas Finland specifies con-
tinuing education and training. Iceland and Sweden do not have requirements for continuing competence for their nurses. The Faroe
Islands and Greenland do not address continuing competencies in their regulations.
Practice
Information about authorized nursing practices was available for Greenland and Sweden but not publicly available for other Nordic
countries. In Sweden, nurses may prescribe medications if they complete a pharmacology/disease control course and midwives can
prescribe contraceptives. Greenland grants nurses and midwives the authority to prescribe medications, refer patients, and diagnose
illnesses in emergencies.
Discipline
In terms of discipline, the following actions are commonly taken in the Nordic region: suspension, revocation or denial of license, warn-
ings, restriction on practice, probation, fine or civil penalty, practice limitation with or without probation, imprisonment, intensified
supervision, and restricted registration.
Western and Central Europe
Western and Central Europe are comprised of Andorra, Austria, Belgium, the Czech Republic, France, Germany, Hungary, Ireland, Italy,
Liechtenstein, Luxembourg, Malta, Monaco, the Netherlands, Poland, Portugal, San Marino, Slovakia, Slovenia, Spain, Switzerland, and
the United Kingdom. Of those 22 countries, Andorra, Liechtenstein, Monaco, San Marino, Switzerland, and the United Kingdom are
the only countries that are not part of the EU. As of January 31, 2020, the United Kingdom has left the European Union; the data in
this report reflects its prior status as a EU member.
Regulation and Governance
Of the 22 Western and Central European countries, nine maintain separate and independent nursing councils, while the other 11 defer
to their Ministry of Health for nursing regulations. Jurisdictions whose nursing professionals are governed by an independent regula
-
tory body are Andorra, Ireland, Italy, Malta, Poland, Portugal, Slovakia, Spain, and the United Kingdom. Jurisdictions whose nursing
professionals are governed by a larger agency body are Austria, Belgium, the Czech Republic, Hungary, Liechtenstein, Luxembourg,
Monaco, the Netherlands, San Marino, Slovenia, and Switzerland.
In the remaining two countries, France and Germany, responsibility for the nursing profession functions somewhat differently.
In both countries, there is a single, national law enacted uniformly in each state or region (France refers to these as “departments”), but
responsibility for administering the laws, including maintaining the registry, is delegated to a regulatory body at the state or departmental
level. In France, including in France’s overseas departments, this is done by a regional branch of the national Ordre des Infermiers (Order of
Nurses), which functions independently from other professions. In Germany, these state regulatory bodies administer multiple disciplines.
Governing bodies across Western and Central Europe, whether independent or governed by a larger agency, hold the authority
to administer nursing laws and regulations, take disciplinary actions, license and register nursing professionals, and make decisions
regarding scope of practice. However, only 59% of jurisdictions hold the authority to create nursing legislation. Some governing bod
-
ies also have powers to handle labor matters, financial matters, inspection, accreditation, and approval of nursing education programs,
offer modifications and opinions on legal acts and laws, and act in an advisory role to a minister of health. Others include disciplinary

58 Journal of Nursing Regulation
matters (the Czech Republic, France, Liechtenstein, Luxembourg, and Malta); education and training matters (Liechtenstein, Monaco,
and San Marino); and financial and budgetary matters (Andorra, the Czech Republic, and Luxembourg).
Regarding the NRBs’ mandates, all but Portugal maintain a mission of public protection. Promotion of the nursing profession
is also part of the mandate in a majority of jurisdictions. However, fewer than half include labor and workforce issues.
NRB Composition
The number of members on NRBs ranges from seven to 153 members. The jurisdictions with both the greatest and fewest number of
members are both independent bodies. Portugal has 153 members, whereas Italy has only seven members (Table 19).
TABLE 19
Number of Members on Nursing Regulatory Bodies in Western and Central Europe
Country Number of Members
Italy 7
Andorra 9
United Kingdom 12
Malta 14
Ireland 23
Czech Republic 61
Belgium 76
Poland 76
Slovenia 122
Portugal 153
Austria Not available
Country Number of Members
France Not available
Germany Not available
Hungary Not available
Liechtenstein Not available
Luxembourg Not available
Monaco Not available
Netherlands Not available
San Marino Not available
Slovakia Not available
Spain Not available
Switzerland Not available
Where information is publicly available about the composition of Western and Central European regulatory bodies, most coun-
tries (n = 15) include nurses and midwives. The NRBs for France, Italy, and Portugal are composed entirely of nurses. Belgium, the
Czech Republic, Luxembourg, Slovenia, and the United Kingdom all include physicians on their NRB, and Ireland, Malta, and the
United Kingdom include members of the public. In Hungary and Liechtenstein, the regulatory body comprises members of various
health professions, and in Austria and the Netherlands, the regulatory body comprises public servants who may or may not be nurses.
No information is available about the NRB composition of San Marino or Switzerland.
Information about additional requirements or qualifications for those serving on NRBs in Western and Central Europe is not
often publicly available. Belgium requires half of its members to be specialized nurses. Spain provides for specialties to be represented
and also specifies that nurse educators from public and private institutions, as well as representation for retired nurses, employment,
and alternative therapies be members. Portugal sets required minimum nursing experience for its president and members, whereas the
United Kingdom has set forth a code of conduct for its members. France’s national council is elected by its regional councilors, and the
French statute sets out strict guidance for fair representation of genders within its councils.
Licensure and Registration Requirements to Practice
Western and Central Europe recognize authorized nursing professionals who have completed their mandatory education and other
requirements in the grant of a nursing diploma, licensure, certification and/or registration. Information is not publicly available as to
how San Marino authorizes its nursing professionals currently.
Austria, the Czech Republic, France, Germany, Hungary, Italy, Luxembourg, Slovakia, Slovenia, and Spain require passage of a
qualifying examination before a nurse is authorized to practice. Most countries in this region also require proof of language proficiency,
with the exceptions being Austria, Belgium, Hungary, Slovakia, and Spain. A majority of jurisdictions also require some form of evidence
of good moral character. Other requirements for authorization to practice include declaration of physical fitness (Ireland) or indemnity
insurance (Liechtenstein, Switzerland, and the United Kingdom).
Once a nursing professional receives his or her nursing diploma, license, certificate and/or is appropriately registered, a public
database is typically the means by which a nursing professional’s credentials are verifiable. In comparison to Eastern Europe, most
of Western and Central Europe maintain an online public database or registry of nursing professionals. Austria, Belgium, the Czech
Republic, France, Hungary, Ireland, Italy, Luxembourg, the Netherlands, Slovenia, Spain, Switzerland, and the United Kingdom are
among those countries.

www.journalofnursingregulation.com 59Volume 10
•
Special Issue
•
January 2020
Currently, Andorra, Liechtenstein, Malta, and Slovakia only provide the public with access to the information by supplying the
requestor with a newspaper, file, or other type of document stored at the Ministry of Health’s headquarters. It is not clear if these data
are accessible in Monaco or San Marino. Poland and Portugal are rare exceptions and restrict all registry access and related disciplinary
record information.
Nurse Types and Titles
Western and Central Europe employ a breadth of nurse specialty types in addition to nurse, midwife, and nurse assistant roles (Tables
C32 through C34). In terms of general nursing, Hungary and Poland recognize variations in the education of nurses, such as RNs, nurses
holding a bachelor’s degree in nursing, and nurses holding a master’s degree in nursing. Italy recognizes RNs in general care and in
pediatrics. The role of the midwife is recognized in 16 jurisdictions. Jurisdictions that do not appear to specifically recognize midwives
are Belgium, Italy, Poland, Portugal, San Marino, and Switzerland.
Many jurisdictions in this region recognize several specialty nurses. Pediatric and psychiatric/mental health nurses are common, as
are surgical/operating room nurses. Notably, Hungary recognizes occupational health nurses. In addition to recognizing mental health
nurses, the United Kingdom and Ireland both recognize intellectual disability nurses. In addition to nurse specialists and pediatric
nurses, Germany also recognizes geriatric nurses. Only Austria, the Czech Republic, France, Germany, Monaco, and Slovenia recognize
nursing assistants, auxiliary nurses, nursing technicians, or healthcare assistants.
Education
Education programs for general nurses or RNs have a duration of 3 years in a majority of jurisdictions (Tables 32 through 34). In ju-
risdictions reporting specialty nurse programs, those programs generally have a duration of 1 to 2 years. Specialty nurse programs in
Germany are 3 to 4 years. In Malta, Ireland, Slovakia, and Spain, programs may be 3 years long depending on which educational track
a student has chosen.
Continuing Competence
Lastly, continuing competence/education appears to be a requirement in most Western and Central European countries except in Belgium,
Ireland, Portugal, and Switzerland. There are no clear data whether such a requirement is mandated in Hungary or San Marino.
Practice
Overall, nurses in Western and Central Europe have limited authority to prescribe medications, diagnose illnesses, and refer patients. That
is evident in Spain, where nurses may prescribe medications so long as they have an order of dispensation. Similarly, in Monaco, nurses
may prescribe certain vaccinations and make nursing diagnoses and referrals in emergencies, and in Luxembourg, nurses can prescribe
medications and refer patients only in emergencies. In France, nurses are authorized to renew prescriptions for oral contraceptive drugs,
other prescriptions less than 1 year old, limited medical devices, and nicotine substitutes. Nurses in Poland must complete an additional
course specializing in prescribing medicine and writing prescriptions before he or she can write prescriptions for medications within
doctors’ orders or issue referrals for specific diagnostic tests. In the United Kingdom, nurses must complete nursing council–approved
post-registration qualifications before they can prescribe medications, as they are not granted prescribing rights upon registration. Nurses
may prescribe in Austria in line with a doctor’s previous instructions.
Nurses in the Czech Republic, Malta, Portugal, and Slovakia are completely restricted from prescribing medications. Nurses
are authorized, however, to refer and diagnose patients in Portugal. In Switzerland, nurses may only diagnose illnesses, while nurses
in Ireland and Slovenia may refer patients. For some countries, information on diagnosis and prescribing is lacking entirely, such as in
Germany, Hungary, Italy, and San Marino.
Discipline
In addition to verifying a nursing professional’s credentials, notifications of past or current disciplinary actions are also publicly acces-
sible as part of a nursing registry. In terms of discipline, the following actions are commonly taken in Western and Central Europe:
(a) reprimand, (b) suspension, (c) fine or civil penalty, (d) denial or withdrawal of license, (e) surrender of license, (f) removal or denial
of name from register, (g) revocation, (h) practice limitation, (i) probation, (j) censure, and (k) warnings. Data on specific disciplinary
measures are lacking in Hungary, Portugal, and San Marino.

60 Journal of Nursing Regulation
The Middle East
F
or purposes of the following analysis, Middle Eastern jurisdictions include Armenia, Azerbaijan, Bahrain, Georgia, Iran, Iraq,
Israel, Jordan, Kuwait, Lebanon, Oman, Palestine, Qatar, Saudi Arabia, Syrian Arab Republic, United Arab Emirates, and Yemen.
As Cyprus is a member of the European Union, analysis of Eastern Europe included Cyprus.
Regulation and Governance
The majority of the regulatory bodies that govern nursing in the Middle Eastern jurisdictions are a cooperation between a larger agency
and an independent body. Georgia does not have a regulatory body that oversees nursing, and there is no information publicly available
about the nursing regulatory body in Palestine.
In many jurisdictions, an authorizing agency body of the national government such as the Ministry of Health or general medical
or health authority is the governing regulatory body. This is the case in Armenia, Azerbaijan, Bahrain, Iraq, Kuwait, Palestine, Qatar,
Saudi Arabia, and Yemen. Lebanon and the United Arab Emirates have NRBs that are independent of those for other health professions.
The respective Ministry of Health, in cooperation with a medical or health authority or council governs the nursing profession in
Iran, Israel, Jordan, Oman, and the Syrian Arab Republic. In Israel, The Nursing Administration within the Ministry of Health governs the
nursing profession. In Iran, the Ministry of Health and Medical Education works in conjunction with the Nursing Board of the Ministry
of Health, which approves nurse education institutions, whereas the Ministry holds other powers. In Oman, the Directorate General of
Nursing Affairs, under the Ministry of Health, governs the profession. The Syrian nursing profession is regulated by its Council of the
Branch, which is a regional body under the Ministry of Health. Regulations and standards are set through the Ministry of Health, but
the regional Council of the Branch executes registrations and approves the applicant for practice of the profession. The nursing profes
-
sion in Jordan is regulated by the Ministry of Health, the Jordanian Nursing Council, and the Jordanian Nurses and Midwives Council.
All regulatory bodies license nursing professionals and all (except for Kuwait) make decisions about authorizing practice respon
-
sibilities. Most (except for Kuwait and Oman) hold the responsibility to administer laws and regulations. The Yemeni Medical Council
and the Azerbaijan Republic Ministry of Public Health hold additional authority to participate in nursing labor and work-related
matters. Most jurisdictions except for Iran, Palestine, Syria, and the United Arab Emirates also discipline nurses. In just over half of
the Middle Eastern countries (Armenia, Azerbaijan, Bahrain, Iran, Israel, Jordan, Lebanon, Qatar, and the United Arab Emirates), the
NRB also has the ability to create legislation.
No information is publicly available about the mandate, or mission, of the Palestinian regulatory body. Of the fifteen other Middle
Eastern countries with an NRB, all state that public protection is a part of their mandate. Eight countries (Armenia, Azerbaijan, Iran,
Israel, Jordan, Lebanon, Oman, and Saudi Arabia) also promote the nursing profession, and five (Azerbaijan, Jordan, Lebanon, Syria,
and Yemen) also handle nursing workforce and labor matters.
NRB Composition
Most members of the multidisciplinary bodies are either positioned in an ex officio manner or nominated by their profession and approved
by the government; however, members of the Saudi Arabia Health Commission and the Qatar Council for Healthcare Practitioners are
approved and appointed.
There are between five and 20 members on NRBs across the Middle East (Table 20). In Israel, representatives must be Israeli citi
-
zens and residents and must possess a satisfactory background and review. In other jurisdictions, a member must be a registered nursing
professional who has practiced for a minimum number of years. In Qatar, the multidisciplinary Council consists of medical professors,
deans of medical schools, and officials from various medical organizations and medical oversight boards.

www.journalofnursingregulation.com 61Volume 10
•
Special Issue
•
January 2020
TABLE 20
Number of Members on Nursing Regulatory Bodies in the Middle East
Country Number of Members/
Representatives
Syrian Arab Republic 5
Qatar 7
Armenia 10
Jordan 10
Iran 11
Lebanon 12
Azerbaijan 14
Saudi Arabia 20
Bahrain No data
Country Number of Members/
Representatives
Georgia No data
Iraq No data
Israel No data
Kuwait No data
Oman No data
Palestine No data
United Arab Emirates No data
Yemen No data
Licensure and Registration Requirements to Practice
All regulatory bodies license nursing professionals. Eleven of the 17 Middle Eastern jurisdictions require a qualifying examination for
certain nurse types leading to authorization to practice in the profession (Table 21).
TABLE 21
Examination Requirements by Jurisdiction and Nurse Type in the Middle East
Jurisdiction Nurse Type Requires
Qualifying
Examination
Armenia RN Yes
Nurse Ye s
Nurse assistant Yes
Azerbaijan Nurse-midwife Yes
Midwife Yes
Auxiliary midwife Yes
Bahrain General nurse Yes
Practical nurse Yes
Specialist nurse Yes
Clinical nurse specialist Yes
Midwife Yes
Iran General nurse/nurse technician Yes
Iraq Midwife Yes
Nurse Ye s
Israel Advanced practice RN Yes
RN Yes
Practical nurse Yes
Midwife Yes
Public health nurse Yes
Academic registered lactation
consultant
Yes
Jurisdiction Nurse Type Requires
Qualifying
Examination
Lebanon RN Yes
RN (technique superior) Yes
Nurse Ye s
Palestine Nurse Ye s
Midwife Yes
Qatar Registered General Nurse Yes
Registered Nurse Yes
Registered Midwife Yes
Clinical Nurse Specialist No
Nurse Practitioner No
Nurse Trainee No
Saudi Arabia Nurse Yes
Nurse specialist Yes
Nursing assistant Yes
United Arab
Emirates
Practical nurse Yes
RN Yes
Advance practice nurse Yes
Practical midwife Yes
Note. RN=registered nurse.
For nurses wishing to practice in the Middle East, a language proficiency examination is required in Iran and Israel. Information
is not publicly available as to whether a language proficiency examination is required in other Middle Eastern jurisdictions. All Middle
Eastern jurisdictions require some form of evidence of good moral character in order to practice within the profession.
Overall, nearly all nurses in this region must take a qualifying examination before they are authorized to practice. In addition to
the Type 1 Practice Nurse in Georgia, for which an examination is not required, Iran’s practical nurse, nurse anesthetist, and operating

62 Journal of Nursing Regulation
room nurse do not require an examination. Additionally, Jordan’s RN, associated nurse or practical nurse roles, Qatar’s clinical nurse
specialist or nurse practitioner roles, and Oman’s nurse and midwife roles do not require an examination.
In the Middle East, an NRB may grant authorization to practice in the nursing profession by license, registration, or registration
followed by a license (Table 22). Authorization to practice may also be granted by a certification followed by registration, or nurses may
simply be authorized to practice when their education and training has been successfully completed. The 17 Middle Eastern jurisdic
-
tions are split as to the means by which they grant authorization to practice nursing.
TABLE 22
Authorization to Practice Nursing in the Middle East
Country How Are Nurses Authorized to Practice?
Armenia On completion of education
Azerbaijan Certification certificate and registry
Bahrain Licensure
Georgia On completion of education
Iran Registration
Iraq Licensure and registration
Israel Registration
Jordan Licensure
Kuwait Licensure
Country How Are Nurses Authorized to Practice?
Lebanon Licensure and registration
Oman Licensure and registration
Palestine Licensure
Qatar Licensure and Registration
Saudi Arabia Registration
Syria Registration
United Arab Emirates Licensure and registration
Yemen Licensure
To identify and verify those nursing professionals who are authorized to practice, some jurisdictions retain a register containing the
names of those authorized. Sometimes, this register is made available to the public. In the Middle East, four jurisdictions that strictly
grant authority by license (Palestine, Yemen, Kuwait, and Jordan) do not offer a publicly available register. The exception to this rule is
Bahrain, whose registry of nursing professionals is published online. Armenia does not offer a publicly available registry. In Lebanon, the
Order of Nurses publishes public information on its website related to the number of nurses per nursing degree and the distribution of
those nurse across different healthcare sectors; however, specific identities of nursing professionals are not publicly included. Remaining
Middle Eastern jurisdictions are divided as to whether a register of nursing professionals is freely available to the public.
Nurse Types and Titles
The Middle East uses common nurse types such as RNs, practical nurses, and midwives; however, some nurse types and categories are
very detailed (Tables C35 through C38). For example, Israel recognizes a particularly specialized nurse—the academic registered lacta
-
tion consultant. There are two types of registered nurses, RNs and technique superior registered nurses, in Lebanon. The four types of
nurse specialists in Saudi Arabia are General Specialists 1 and 2 and First Specialists 1 and 2. These nurse specialists are categorized by
education, training, and competence. For instance, Nurse Specialist 1 requires successful completion of a bachelor’s degree program in a
specialty for entry into the Nurse Specialist 1 program, whereas a master’s degree or equivalent in a specialty is required for entry into a
Nurse Specialist 2 program. Furthermore, 2 years of post–master’s degree experience in nursing is required for First Specialist 1 program
entry, and 3 years of post–master’s degree experience in nursing is required for First Nurse Specialist 2 program entry.
Georgia has two types of general nurse, a Type 1 practice nurse and a Type 2 practice nurse. The Type 1 practice nurse requires
completion of secondary education before program entrance, whereas and Type 2 practice nurse requires passage of the National Entrance
Examination.
Oman requires the demonstration of English language proficiency including admission interviews held in both Arabic and English
languages for psychiatric nurses, infectious disease nurses, and pediatric nurses.
Most Middle Eastern jurisdictions also recognize a general midwife and some form of nurse assistant. In Bahrain, Iran, Israel,
Jordan, and the United Arab Emirates, a nursing assistant is also called a Practical Nurse. Jordan has suspended its practical nursing
program from new applicants.
Education
In a majority of jurisdictions, education programs are approved by each jurisdiction’s respective Ministry of Health, Ministry of Education,
or in a cooperation with both. The regulatory boards in Iran, Qatar, and Oman hold exclusive authority to approve nursing education
programs.
Regarding nurse education, requirements vary depending on nurse type (Tables C35 through C38). Overall, general nursing
programs range between 3 to 4 years. In Israel, the core curriculum for the nursing program is 4 years for a degree program and 2.5

www.journalofnursingregulation.com 63Volume 10
•
Special Issue
•
January 2020
years for a diploma program. In addition, each nursing institution may enhance that curriculum. To become a nursing professional in a
specialty, such as an operating room nurse in Iran or a nurse-midwife in Azerbaijan, a minimum of an additional 1 or 2 years of educa
-
tion and training is required.
Continuing Competence
Nearly all jurisdictions in the Middle East require some sort of continuing competence. This requirement varies depending on nurse type
and renewal period. Azerbaijan follows a lifelong learning requirement for nursing professionals, which is similar to EU jurisdictions.
Lebanon is currently in the process of developing continuing competency standards. In general, licensed professionals in the Middle East
may renew their license to practice every 4 to 5 years following successful completion of continuing competence.
Practice
From the limited data, the scope of practice varies depending on nurse type across the Middle Eastern region. In Azerbaijan, a midwife
may diagnose pregnancies and refer patients for additional medical care. In Syria, a nursing professional may perform all urgent medical
assistance only after the arrival of a physician. Furthermore, in Syrian villages and areas where there is no pharmacy, it is permissible
for a nursing professional to sell medicines after obtaining permission from the Ministry of Health. In Qatar, a nurse practitioner may
prescribe medication, and nurse practitioners, registered midwives, and clinical nurse specialists can refer patients to other services.
Discipline
Nearly all Middle Eastern jurisdictions take disciplinary measures against nursing professionals when necessary. Sanctions are more
extensive in some jurisdictions. For example, sanctions in Azerbaijan include a fine or civil penalty, revocation of the authorization to
practice, and a denial of the Certification Certificate. Sanctions in Armenia include a limitation and probation on the professional’s ability
to practice and a denial of authorization to practice. Other sanctions employed in the Middle East include denial of registration, warnings,
remediation, suspension of authorization/license, removal of the professional’s name from the register, reprimands, and imprisonment.
Some jurisdictions enlist broad sanctions. Disciplinary measures in Iran include varying forms of probation, suspensions, and
limitations on practice. Jordan’s regulatory system may implement any and all sanctions because the Ministry of Health disciplines
on matters relating to licensing and the Jordanian Nursing Council disciplines on matters relating to a professional’s specialization
and professional classification. Disciplinary records in a majority of the jurisdictions are not available to the public; however, the Saudi
Arabia Health Commission makes disciplinary records of health professionals public. The Qatar Council for Healthcare Practitioners
has an online registry of nurses, accessible with an account, but it is unclear whether the same registry contains discipline information
or whether that information is available to the public. In Lebanon, disciplinary records are considered strictly confidential.

64 Journal of Nursing Regulation
APPENDIX A
Glossary of Terms
accreditation (accrediting body) A nongovernmental, often voluntary,
peer review process for educational programs that assesses the
quality of an educational program and recognizes programs as
meeting a set of requirements.
advanced practice registered nurse (APRN) A registered nurse who has
a graduate degree and advanced knowledge. There are four catego
-
ries of APRNs: certified nurse-midwife (CNM), certified nurse practi-
tioner (CNP), clinical nurse specialist (CNS), and certified registered
nurse anesthetist (CRNA). These nurses can diagnose illnesses and
prescribe treatments and medications.
African Health Profession Regulatory Collaborative for Nursing and
Midwifery (ARC) A collaborative comprised of 17 African member
nations whose objectives are to support and build nursing and mid
-
wifery capacity to sustain and increase HIV services; advance nurs-
ing and midwifery regulatory frameworks; strengthen nursing and
midwifery organizational capacity and leadership; foster collabora
-
tion; and promote dialogue between member countries.
approval (of education) Official recognition of a nursing education pro
-
gram as meeting the standards established by the appropriate gov-
ernment authority.
Association of Southeast Asian Nations (ASEAN) A 10-member associ
-
ation of Southeast Asian nations whose purposes and aims are to
accelerate the economic growth, social progress and cultural devel
-
opment in the region through joint endeavors in the spirit of equali-
ty and partnership; to promote regional peace and stability through
abiding respect for justice and the rule of law in the relationship
among countries of the region and adherence to the principles of
the United Nations Charter; to promote active collaboration and mu
-
tual assistance on matters of common interest in the economic, so-
cial, cultural, technical, scientific, and administrative fields; to pro-
vide assistance to each other in the form of training and research
facilities in the educational, professional, technical, and administra
-
tive spheres; to collaborate more effectively for the greater utiliza-
tion of their agriculture and industries, the expansion of their trade
(including the study of the problems of international commodity
trade), the improvement of their transportation and communica
-
tions facilities, and the raising of the living standards of their peo-
ples; to promote Southeast Asian studies; and to maintain close and
beneficial cooperation with existing international and regional orga
-
nizations with similar aims and purposes and explore all avenues
for even closer cooperation among themselves.
authorization to practice Authority granted to a nursing professional
allowing that professional to practice nursing within the scope of his
or her respective discipline. This authority is generally granted after
a nursing professional has completed the required education and
training programs within their jurisdiction. A qualifying examination
leading to authorization may also be required.
board of nurses (nursing board) A governmental agency responsible
for regulation of the nursing practice.
Canadian Free Trade Agreement (CFTA) An agreement that applies to
trade, investment, and labor mobility within Canada comprising
14-member provinces and the Canadian federal government. The
Agreement seeks to eliminate barriers in trade and the mobility of
goods, services, investments, and persons within Canada by recon
-
ciling standards and regulatory measures through nondiscriminato-
ry treatment.
Caribbean community (CARICOM) Comprised of 15 Caribbean member
states and five associate Caribbean member states; the overarching
purpose of CARICOM is to encourage and engage in functional co
-
operation between Caribbean nations. CARICOM rests on four main
pillars economic integration; foreign policy coordination; human
and social development; and security.
cease and desist order A document sent to an individual to permanent
-
ly halt purportedly unlawful activity.
censure A reprimand, which could be public or private, for an infraction
or violation.
certified nursing assistant (certified nursing aid) (CNA) A person who
is certified to assist with the delivery of direct nursing care to pa
-
tients. Works under the supervision of a nurse.
certified nurse midwife (CNM) A registered nurse (RN) who has a grad
-
uate degree and advanced knowledge specific to the practice of
midwifery. The CNM is one of four types of advanced practice RNs:
certified nurse midwife (CNM), certified nurse practitioner (CNP),
clinical nurse specialist (CNS), and certified registered nurse anes
-
thetist (CRNA). These nurses can diagnose illnesses and prescribe
treatments and medications.
certified nurse practitioner (CNP) A registered nurse (RN) who has a
graduate degree and advanced knowledge. The CNP is one of four
types of advanced practice RNs: certified nurse midwife (CNM), cer
-
tified nurse practitioner (CNP), clinical nurse specialist (CNS), and
certified registered nurse anesthetist (CRNA). These nurses can diag
-
nose illnesses and prescribe treatments and medications.
certified nurse specialist (CNS) A registered nurse (RN) who has a
graduate degree and advanced knowledge in a specific specialty.
The CNS is one of four types of advanced practice RNs: certified
nurse-midwife (CNM), certified nurse practitioner (CNP), clinical
nurse specialist (CNS), and certified registered nurse anesthetist
(CRNA). These nurses can diagnose illnesses and prescribe treat
-
ments and medications.
certified registered nurse anesthetist (nurse anesthetist) (CRNA) A reg
-
istered nurse (RN) who has a graduate degree and advanced knowl-
edge in the administration of anesthesia. The CRNA is one of four
categories of advanced practice RNs: certified nurse-midwife (CNM),
certified nurse practitioner (CNP), clinical nurse specialist (CNS), and
certified registered nurse anesthetist (CRNA). These nurses can diag
-
nose illnesses and prescribe treatments and medications.
citation order A civil penalty that may affect a nurse’s licensure or reg
-
istration but usually is not related to the nurse’s actions in practice.
compact An agreement between several jurisdictions that allows nurs
-
es from each jurisdiction to work in any participating jurisdiction
without meeting additional requirements.
conditional probation Limitation or restriction of one or more aspects
of practice.
continuing competence (continuing professional development) (con
-
tinuing fitness to practice) Additional education or training follow-
ing initial authorization to practice. It is often required to remain au-
thorized to practice.
credentials In some countries, the abbreviations included in a person’s
title that indicate the achievement of a certain level of education or
training, such as MD for medical doctor.
discipline Review and investigation taken by a regulatory body acting
through its statutory authority after a nurse has or is alleged to have
violated the nursing laws, acts, or regulations. The regulatory body
may take disciplinary action against the nurse’s license.
East, Central, and Southern Africa College of Nursing (ECSACON) An
arm of the East, Central, and Southern Africa Health Community
(ECSA-HC). ECSACON focuses on the areas of nursing and midwife
-
ry. The mandate seeks to promote and strengthen professional ex-
cellence in nursing and midwifery in the region.
East, Central, and Southern Africa Health Community (ECSA-HC) A
nine-member intergovernmental health organization that fosters
and promotes regional health cooperation among member states.
Appendices

www.journalofnursingregulation.com 65Volume 10
•
Special Issue
•
January 2020
European Union (EU) A union of 28 member European countries
whose goals and values are to promote peace, its values, and the
well-being of its citizens; to offer freedom, security, and justice with
-
out internal borders; to offer sustainable development based on bal-
anced economic growth and price stability, a highly competitive
market economy with full employment and social progress, and en
-
vironmental protection; to combat social exclusion and discrimina-
tion; to promote scientific and technological progress; to enhance
economic, social, and territorial cohesion and solidarity among EU
countries; to respect its rich cultural and linguistic diversity; and to
establish an economic and monetary union whose currency is the
euro.
fitness to practice Having the skills, knowledge, competence, health,
and character to practice within the nursing profession. Evidence of
moral character such as criminal background checks and references
may be included.
gazette (national gazette) An official publication by a government.
governance The means by which nurses are regulated in a jurisdiction,
including the laws and regulations that apply to nurses and the or
-
ganization with the authority to enforce these regulations.
independent governing body (independent body) An organization that
operates independently from bodies that regulate other professions.
jurisdiction The country, state, province, or other geographically delin
-
eated region in which a single, uniform set of nurse laws applies.
license/licensure A method by which regulatory bodies grant a nurse
authorization to practice. Nurses must meet certain criteria to re
-
ceive a license and are sometimes required to renew the license af-
ter a certain period of time.
licensed practical nurse (licensed vocational nurse) (LPN) (LVN) An in
-
dividual who has completed a state-approved practical or vocational
nursing program, passed the National Council Licensure Examina
-
tion for Practical Nurses (NCLEX-PN), and is licensed by a state
board of nursing to provide patient care. Normally works under the
supervision of a registered nurse, advanced practice registered
nurse, or physician.
mandate The action or actions an organization is authorized and ex
-
pected to take.
medication aid (certified medication aid/assistant) (MA-C) A person
who is certified to administer medication under the supervision of a
nurse.
Ministry of Education A ministry of government that has responsibility
for multiple areas of education and education professions.
Ministry of Health A ministry of government that has responsibility for
multiple areas of healthcare and health professions.
mobility The ability of nurses to work across state, province, or country
borders.
multidisciplinary body An entity that regulates many areas or many
professions, such as a Ministry of Health or Ministry of Education.
mutual agreement An agreement between two jurisdictions that allows
nurses from each jurisdiction to work in either jurisdiction without
meeting additional requirements.
national examination A nationally required examination for nurse
licensure.
National Council Licensure Examination (NCLEX) A national licensure
examination developed by the National Council of State Boards of
Nursing (NCSBN) for registered nursing (NCLEX-RN) and practical/
vocational nursing (NCLEX-PN) in the United States, the U.S. territo
-
ry members, Canada, and U.S. associate members.
nursing council (nursing board) (board of nurses) A governmental
agency responsible for regulation of the nursing practice.
nursing diagnosis An evidence-based clinical judgment that allows a
nurse to develop a care plan and select nursing interventions.
Nurse Licensure Compact (NLC) An agreement allowing a nurse to
have one multistate license with the ability to practice in the home
state and other member compact states.
nursing register (role of nurses) (register of nurses) A list or database
of every nurse currently authorized in a jurisdiction.
probation Limitation of practice.
public member A member of the regulatory body that does not belong
to the profession that the body regulates.
qualifying examination An examination for nursing licensure.
register/registration A method by which regulatory bodies grant a
nurse authorization to practice. Nurses must meet certain criteria to
join the register and are sometimes required to renew their registra
-
tion after a certain period of time.
registered nurse (RN) An individual who has graduated from a state-
approved school of nursing, passed the National Council Licensing
Examination for Registered Nursing, and is licensed by a state board
of nursing to provide patient care.
regulatory body (governing body) The organization, usually a branch of
the government, that is authorized to regulate nurses within a
jurisdiction.
remediation Requirements that a nurse must accomplish to reinstate
authorization to practice after it has been suspended.
reprimand A public and formal censure administered to a nurse by the
appropriate governing body.
revocation Permanent removal of a nurse’s authorization to practice.
sanction A penalty or punishment against a nurse’s authorization to
practice.
scope of practice The tasks and procedures that a nurse is qualified
and authorized to carry out based on his or her level of training.
Southern Common Market (MERCOSUR) An economic and political
bloc encompassing certain South American and Caribbean nations.
The main objective of MERCOSUR is to promote a commonality in
the process of generating business and investment opportunities by
integrating the national MERCOSUR economies into the internation
-
al market.
specialist nurse A nurse who is part of a consulting team and provides
a specific type of advice, counselling, and care. In some jurisdic
-
tions, a specialist nurse is a type of advanced practice registered
nurse.
summary suspension Emergency action to remove a nurse’s authoriza
-
tion to practice in order protect the health safety and welfare of the
citizens of the state.
suspension Removal of a nurse’s authorization to practice for a period
of time.
telehealth The practice of healthcare in which the patient and provider
are not in the same physical location, through the use of
telecommunications.
World Health Organization (WHO) An agency of the United Nations
that seeks to direct and coordinate international health within the
United Nations system, supporting countries and work mainly in the
areas of health systems; health through the life course; noncommu
-
nicable and communicable diseases; preparedness, surveillance,
and response; and corporate services.

66 Journal of Nursing Regulation
APPENDIX B
Jurisdictions Not Included in Data Analysis
1
In the early 21st century, all five French overseas entities listed here as sub-jurisdictions became French regions and were made part of France proper.
France maintains the nursing registry for all five sub-jurisdictions.
2
The following British territories do not share a nursing registry with the United Kingdom, but rather have their own: Anguilla, Bermuda, British
Virgin Islands, Cayman Islands, and Turks & Caicos.
3
“Morocco and The Popular Front for the Liberation of Saguia el Hamra and Rio de Oro (Polisario) dispute each other’s claims of sovereignty over ter-
ritories in Western Sahara. Thus, the governmental authority—and authority over professional groups such as nursing—remain unresolved the terri-
tory. See U.S. Department of State. (2003, March 31). Western Sahara. https://2009-2017.state.gov/j/drl/rls/hrrpt/2002/18292.htm
TABLE B1
Jurisdiction not included in Data Analysis
Sub-jurisdictions of Australia, France, New Zealand, and the United Kingdom that were not included because they were part of another
country. jurisdictions of Central America and Africa were not included because sufficient data could not be gathered
Region Jurisdiction or Sub-jurisdiction
Australia Norfolk Island
Pitcairn Islands
France
1
French Guiana
Guadeloupe
Martinique
Mayotte
Réunion
New Zealand Niue
Tokelau
The United Kingdom
2
Falkland Islands
Gibraltar
Guernsey
Jersey
Isle of Man
Saint Helena
Region Jurisdiction or Sub-jurisdiction
Central America Panama
Africa Algeria
Angola
Chad
Equatorial Guinea
Guinea-Bissau
Sao Tome and Principe
Senegal
Somalia
South Sudan
Sudan
Western Sahara
3

www.journalofnursingregulation.com 67Volume 10
•
Special Issue
•
January 2020
APPENDIX C
Educational Requirements for Entry into
Nursing Programs by Regions
This appendix comprises tables that outline the duration of nursing programs and the requirements to enter those programs by conti-
nent/region and nurse type (e.g., general nurse, specialist nurse, midwife, nurse assistant).
Africa
TABLE C1
Types of Nurses and Duration of Nursing Program and Requirements for Entry—General
Nurses in Africa
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Benin Nurse No data No data
Botswana RN 3–4 years Higher secondary education
Burkina Faso Nurse No data Successful completion of Grade 12
Burundi RN 2–4 years
Technical school (nursing): 2
years
Technical school (university ac
-
cess nursing): 3–4 years
Passage of lower secondary education, or higher secondary
education with passing examination for university
Cape Verde General nurse 4 years No data
Primary nurse
(3 levels)
3–4 years
Level 1: 4 years of nursing educa
-
tion and training in addition to
master’s level education
Level 2: 3 years of nursing educa
-
tion and participation in scientif-
ic/ professional article
Level 3: 3 years of nursing educa
-
tion, participation in 2 scientific
articles, and participation in sci
-
entific/ professional activities
4 years of previous nurse training
Cameroon Graduate nurse 3 years Complete entrance examination to training school; com
-
plete minimum of Grade 12 education.
External candidates must be aged ≤25 years on December
31 of the year of the application and complete an entrance
examination approved by Ministry of Health
Congo, Democratic
Republic of
No data No data No data
Côte d’Ivoire Nurse No data No data
Djibouti Nurse 3 years Completion of secondary school
Egypt Nurse 3 years Completion of high school
Ethiopia Nurse Program comprises 1650 theory
hours and 420 hours of intern
-
ship course modules in hospital
Must have successfully completed at least Grade 10 and the
minimum requirements of the Ministry of Education
Bachelor of
nursing
4 years Successfully completed Grade 12 and possess the mini
-
mum requirements or directives of the Ministry of
Education
Gabon Nurse 3 years Completion of Grade 12
Gambia RN 3 years GCE O Level: 5 credits that must include English, science,
and three other academic subjects; OR Senior Secondary
School Certificate of Education: 4 credits that must include
English, science, and two other academic subjects
Enrolled nurse 2 years

68 Journal of Nursing Regulation
TABLE C1 (continued)
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Gambia
(continued) Bachelor of
nursing
2.5–4 years
Duration is dependent on educa
-
tional tract
4-year BSN program requires Senior Secondary School Cer
-
tificate with credit passes in English language and mathe-
matics and any other three science courses (biology, chem-
istry, physics, general sciences, or further mathematics)
RN to BSN program requires candidates to be an RN for a
minimum of 2 years, in addition to credit passes in courses,
as above.
Guinea Nurse 3 years Minimum education of Grade 12 (high school)
Ghana RN 3 or 4 years, depending on 3-year
diploma or 4-year degree
Age limit, 18–35 years. Depending on program: Overall ag
-
gregate score of 30 or better in six subjects comprising
three core and three electives, or overall aggregate score of
24 or better in six subjects comprising three core and three
electives.
Lesotho General nurse/
nurse technician
3 years Licensure, credentialing and registration
Liberia RN Has completed prescribed educa
-
tion and training from accredited
institution
Minimum high school education (Grade 12)
Graduate nurse Has graduated from accredited
program.
No data
Madagascar Nurse 3 years Completion of Grade 12 (high school)
Master’s in
nursing
No data Must have a bachelor’s degree; state diploma in nursing or
midwifery or other equivalent recognized diplomas; must
have at least 3 years of and pass an entrance examination
Malawi Registered nurse
midwife
4 years GCE O level with six credits in science subjects
Nurse midwife
technician
3 years GCE O level with three credits in science subjects
Mauritania Nurse No data Completion of Grade 12
Mauritius Registered gen
-
eral nurse
3 years High school certificate with one science subject
Enrolled nurse 2 years No data
Morocco RN No data Completion of high school and certificate of health includ
-
ing vaccinations (students are entitled to vaccine program
through Government Health Authority); science diploma if
applying for entry into the Higher Institutes of Nursing and
Health Professions
Mozambique RN No data Completion of Grade 12
Namibia RN 3–4 years No data
Enrolled nurse No data No data
Niger General nurse 3 years Completion of Grade 10
Nigeria General nurse No data Must be aged between 18–35 years and maintain five credit
passes in mathematics, English, physics, chemistry, and bi
-
ology. Any student with foreign examination board result(s)
is expected to submit an evaluation report or equivalent
grading.
Post-basic nurse No data Only students who commenced their basic education be
-
fore the year 2006 can be considered for indexing with the
same entry qualifications accepted during their entry into
basic program.
Rwanda Registered gen
-
eral nurse
3–4 years High school education with successful completion of biolo
-
gy, chemistry, physics, and mathematics
Associate nurse 3 years 3 years of secondary school
South Africa General nurse No data No data
Professional RN 4 years Completion of high school with successful completion of
specific subjects, which vary by university
Enrolled nurse 2 years No data
Tanzania RN 3 years Applicants must successfully pass subjects of biology,
chemistry, and physics
Enrolled nurse 2 years Applicants must successfully pass subjects of biology,
chemistry, and physics.

www.journalofnursingregulation.com 69Volume 10
•
Special Issue
•
January 2020
TABLE C1 (continued)
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Togo State-certified
nurse
3 years No data
Tunisia Nurse 3 years Tunisian nationals must be aged ≥17 years; up to date on
their vaccinations; and must pass an entrance examination.
Foreign applicants are subject to selection examinations
and must present a photocopy of their nursing diploma and
a record of their nursing program of studies and course
hours and evaluations
Zambia RN 3 years Applicants must be in possession of a Cambridge or equiv
-
alent certificate with a pass in English and four other sub-
jects, three of them being general science, mathematics
and biology; or the candidate is the holder of a certificate to
the effect that he or she has been a medical assistant for 3
years and has been working as such continuously for at
least 1 year; attains the age of 17 years
Enrolled nurse 2 years The candidate meets the following educational require
-
ments: submits Form II or Form III with passes in English,
one science subject, and two other subjects; attains the age
of 17 years; passes a medical examination
Zimbabwe Registered gen
-
eral nurse
3–4 years GCE at O Level taken at the end of Grade 11 with grades A
to C in at least five subjects, including English language and
a science
State-certified
nurse
2 years (previously) as state-cer
-
tified nurses are no longer
trained.
Not applicable; state-certified nurses are no longer trained
in Zimbabwe, but some remain in the workforce.
Note. BSN=bachelor of science in nursing; GCE=General Certificate of Education; O Level=ordinary level; RN=registered nurse.
TABLE C2
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Specialty
Nurses in Africa
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Botswana Psychiatric nurse 2 years Diploma in nursing
Family nurse
practitioner
2 years Diploma in nursing
Community health
nurse
2 years Diploma in nursing
Cape Verde Nurse specialist 4 years initial nursing education/
training in addition to participation
in scientific/professional articles
and presentations, followed by ap
-
proval by competition
Participation in at least 4 actions of health promotion and
prevention of diseases within communities, presentation
of clinical cases; participation in technical/scientific activi
-
ties; or obtaining degree of specialty in nursing
Cameroon Reproductive health
nurse
2 years Holds state nursing diploma, has practiced for 2 years,
and completes entrance examination approved by the
Ministry of Health
Ophthalmic nurse 2 years Holds state nursing diploma, has practiced for 2 years,
and completes entrance examination approved by the
Ministry of Health
Nurse anesthetist 2 years Holds state nursing diploma, has practiced for 2 years,
and completes entrance examination approved by the
Ministry of Health
Mental health nurse 2 years Holds state nursing diploma; has practiced for 2 years;
and completes entrance examination approved by the
Ministry of Health
Ethiopia Master’s nurse 2–2.5 years Bachelor of nursing or midwifery degree, 2 years’ work
experience, and successful passing of a university-de
-
signed entrance examination

70 Journal of Nursing Regulation
TABLE C2 (continued)
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Gambia Community health
nurse
2 years No data
Master’s in nursing No data Completion of BSN program
Ghana Nurse practitioner No data No data
Psychiatric nurse 3 years (diploma) or 4 years
(degree)
Age limit is 18–35 years; overall aggregate score of 30 or
better in six subjects comprising three core and three elec
-
tives; or overall aggregate score of 24 or better in six sub-
jects comprising three core and three electives
Public health nurse Completion of nursing program,
followed by 1 year post-basic
training
Holds RGN, RMN, RM, or RCN credential. Service require
-
ment: Mandatory 1-year rotation/internship with National
Service; 3 years’ experience in a relevant basic nursing
area; or 2 years’ experience after nurse internship.
Registered mental
health nurse
3 years Age limit is 18–35 years; overall aggregate score of 30 or
better in six subjects comprising three core and three elec
-
tives; or overall aggregate score of 24 or better in six sub-
jects comprising three core and three electives
Registered commu
-
nity nurse
Training as nurse, followed by 1
year post-basic training/education.
Holds RGN, RMN, RM, or RCN credential. Service require
-
ment: Mandatory 1-year rotation/internship with National
Service; 3 years’ experience in a relevant basic area or 2
years’ work experience upon a request from a facility after
internship.
Pediatric nurse Training as nurse, followed by
post-basic education/training
Holds RGN, RMN, RM, or RCN credential. Service require
-
ment: Mandatory 1-year rotation/internship with National
Service; 3 years’ experience in a relevant basic area or 2
years’ work experience upon a request from a facility after
internship.
Ophthalmic nurse Completion of nursing program,
followed by 1 year post-basic train
-
ing/education
Holds RGN, RMN, RM, or RCN credential. Service require
-
ment: Mandatory 1-year rotation/internship with National
Service; 3 years’ experience in a relevant basic area or 2
years’ work experience upon a request from a facility after
internship.
Oncological nurse 3 years (diploma) or 4 years
(degree)
Age limit is 18–35 years; overall aggregate score of 30 or
better in six subjects comprising three core and three elec
-
tives; or overall aggregate score of 24 or better in six sub-
jects comprising three core and three electives
Critical care nurse/
perioperative nurse
Completion of nursing program
followed by 1 year post-basic train
-
ing/education
Holds RGN, RMN, RM, or RCN credential. Service Require
-
ment: Mandatory 1-year rotation/internship with National
Service; 3 years’ experience in a relevant basic area or 2
years’ work experience upon a request from a facility after
internship.
Lesotho Theater nurse 1 year Completion of a general nursing program
Nurse anesthetist 1 year Completion of a general nursing program
Nurse clinician 2 years Completion of a general nursing program
Liberia Nurse anesthetist No data No data
Licensed practical
nurse
No data Completion of prescribed education and training from ac
-
credited institution
Ophthalmic nurse No data Must be an RN
Madagascar Nurse specialist 2 years Applicants must hold a bachelor’s degree in secondary ed
-
ucation and the state diploma of nurse or midwife or other
recognized equivalent diploma and have at least 3 years
of professional experience. For those in public service, at
least 4 years of effective service in the public sector as a
nurse/midwife.
Mauritius Registered mental
health nurse
5 years High school certificate with one science subject
Mozambique Nurse specialist No data Must be an RN
Rwanda Registered mental
health nurse
3–4 years High school education with successful completion of biol
-
ogy, chemistry, physics, and mathematics
South Africa Nurse specialist 1 year Must be an RN with at least 2 years of experience in the
area of specialty

www.journalofnursingregulation.com 71Volume 10
•
Special Issue
•
January 2020
TABLE C2 (continued)
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Tunisia Psychiatric nurse The general nursing diploma pro
-
gram is 3 years; additional training
for psychiatric concentration may
be required.
Tunisian nationals must be aged ≥17 years; be up to date
on their vaccinations; and pass an entrance examination.
Foreign applicants are subject to selection examinations
and must present a photocopy of their nursing diploma
and a record of their nursing program of studies and
course hours and evaluations.
Nurse anesthetist The general nursing diploma pro
-
gram is 3 years; additional training
for anesthetist concentration may
be required.
See Tunisian requirements previously listed
Public health nurse 3 years See Tunisian requirements previously listed
Zimbabwe Post-basic nurse 6 months–1 year Must be an RGN
Note. RCN=registered certified nurse; RGN=registered general nurse; RMN=registered midwife-nurse; RM=registered midwife; RN=registered
nurse.
TABLE C3
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Midwives in
Africa
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Benin Midwife No data No data
Botswana Registered
midwife
2 years Diploma in nursing
Burkina Faso Midwife 3 years Successful completion of Grade 12
Burundi Midwife 3 years Grade 12 education
Cameroon Qualified wise
woman
3 years Age of 18–30 years on January 1 of the current year; complete entrance ex
-
amination to schools approved by the Ministry of Public Health; and hold a
bachelor’s degree in nursing or equivalent
Central African
Republic
Midwife No data Minimum Grade 12 education (high school)
Comoros Midwife 3 years Minimum high school education to begin training
Congo, Democratic
Republic of
Nurse midwife 3 years Minimum of Grade 12 education before beginning training
Wise woman 3 years Minimum of Grade 12 education to begin training
Congo, Democratic
Republic of
Midwife 3 years Minimum of high school education in order to begin midwife training/
education
Côte d’Ivoire Midwife 3 years Completion of Grade 12
Djibouti Midwife 3 years Completion of secondary school
Egypt Midwife No data No data
Eritrea Midwife No data No data
Nurse-midwife No data No data
Ethiopia Midwife 3–4 years Completion of Grade 12 and satisfaction of minimum requirements or direc
-
tives of the Ministry of Education
Gabon Midwife 3 years Completion of Grade 12
Nurse-midwife No data Completion of Grade 12
Gambia Registered
midwife
1.5 years Applicant must be an RN with 2 years’ work experience and must have at
-
tained the West African Senior Secondary School Certificate of Education,
including 4 credits of English, science, and two other academic subjects.
Nurse midwife No data No data
Ghana Registered
midwife
3 years Age limit is 18–35 years. Depending on program: Overall aggregate score of
30 or better in six subjects comprising three core and three electives, or
overall aggregate score of 24 or better in six subjects comprising three core
and three electives.
Guinea Midwife 3 years Minimum Grade 12 education (high school)
Lesotho Midwife 1 year General nursing is a prerequisite to midwifery. Licensure, credentialing, and
registration are required.

72 Journal of Nursing Regulation
TABLE C3 (continued)
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Liberia Registered
midwife
3 years Minimum high school education (Grade 12)
Registered
nurse-midwife
3 years Minimum high school education (Grade 12)
Certified
midwife
3 years Minimum high school education (Grade 12)
Trained tradi
-
tional midwife
Has completed
training at the
community level
No data
Mali Midwife 3 years Completion of Grade 12 education
Mauritania Midwife 3 years Completion of Grade 12 education (high school)
Mauritius Midwife 2 years Completion of Grade 10 education
Morocco Midwife 3 years Completion of Grade 12 education (high school)
Mozambique Midwife 4 years Completion of Grade 12 education (high school)
Namibia Registered
midwife
1 year Must be an RN and must have completed a general nursing program
Enrolled
midwife
No data No data
Niger General midwife 3 years Completion of Grade 12th education
Nigeria Midwife No data Age of 18–35 years and maintain five O Level credit passes in mathematics,
English, physics, chemistry, and biology. Any student with foreign examina
-
tion board result(s) is expected to submit an evaluation report or equivalent
grading from the Federal Ministry of Education along with the result.
Rwanda Registered
midwife
3–4.5 years High school education with successful completion of biology, chemistry,
physics, and mathematics
Tunisia Wise woman/
midwife
No data Tunisian nationals must be aged ≥17 years; be up to date on their vaccina
-
tions; and pass an entrance examination. Foreign applicants are subject to
selection examinations and must present a photocopy of their nursing di
-
ploma and a record of their nursing program of studies and course hours
and evaluations.
Zambia Registered
midwife
1 year Candidate must possess the former Standard VI Certificate or a Form II Cer
-
tificate; attain the age of 17 years; and pass a medical examination
Enrolled
midwife
No data See Zambia requirements previously listed
Note. O Level=ordinary level; RN=registered nurse.
TABLE C4
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Assistant
and Auxiliary Nurses in Africa
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Burundi Auxiliary nurse 2–4 years
Technical school (nursing): 2 years
Technical school (university access
nursing): 3–4 years
No data
Cape Verde Nurse assistant 3–4 years No data
Cameroon Medical technician 3 years Bachelor’s degree or certificate equivalent except
in religion; external candidates (aged up to 25
years on the year of the competition); and com
-
plete entrance examination to schools approved
by the Ministry of Public Health
Comoros Auxiliary midwife No data Minimum high school education
Congo, Democratic Re
-
public of
Auxiliary midwife No data Minimum high school education
Djibouti Assistant nurse 2 years Completion of secondary school
Assistant midwife 2 years Completion of secondary school

www.journalofnursingregulation.com 73Volume 10
•
Special Issue
•
January 2020
TABLE C4 (continued)
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Ethiopia Healthcare giver A total duration of 800 hours, of
which 531 hours are in school
practice and cooperative training
Successfully complete at least Grade 10 general
education and possess the minimum require
-
ments or directives of the Ministry of Education.
Nursing assistant A total of 1,550 hours in theory
and practice or cooperative train
-
ing; 320 hours of internship are
dedicated to related nursing assis
-
tant practice
Successfully complete Grade 10 general education
and possess the minimum requirements or direc
-
tives of the Ministry of Education.
Ghana Nursing assistant 2 years Age of 18–35 years. Depending on institution,
overall aggregate: score of 48 or better in six sub
-
jects, comprising three core and three electives, or
a cut off score of 30 or better in six subjects com
-
prising three core and three electives.
Malawi Community midwife
assistant
1.5 years O Level
Community health
nurse technician
1 year O Level with three credits in science subjects
Psychiatric nurse
technician
1 year O Level with three credits in science subjects
Mauritius Assistant nurse 2 years No data
Niger Nursing assistant 2 years Completion of at least 6 years of school
South Africa Auxiliary nurse 1 year No data
Togo State auxiliary
nurse
3 years No data
Tunisia Nurse aid No data Tunisian nationals must be aged ≥17 years; be up
to date on their vaccinations; and pass an en
-
trance examination. Foreign applicants are subject
to selection examinations and must present a
photocopy of their nursing diploma and a record
of the program of studies followed specifying the
number of course hours per subject per year of
training and evaluations.
The Americas
TABLE C5
Duration of Nursing Program and Requirements for Entry—General Nurses in Canada
Province/Territory Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Alberta RN 4 years 12 years of primary and secondary education;
minimum secondary GPA and subject completion
requirements; criminal record check
LPN 2 years Completion of secondary education
British Columbia RN 4 years No data
LPN No data No data
Manitoba RN 3 years High school diploma and satisfactory completion
of a criminal record check in addition to an adult
and child abuse registry checks
LPN 2 years High school diploma and additional requirements
that vary by school, such as up-to-date immuniza
-
tions, other necessary certifications, and passing a
criminal record and child abuse registry checks
New Brunswick RN Bachelor’s program in nursing or a
2-year program in nursing and a
minimum of 1,125 hours of prac
-
tice in preceding 5 years
Prerequisites that provide a reasonable assurance
of success in the program and the requisite skills
and abilities needed to achieve entry-level
competencies
LPN 2 years High school diploma
Newfoundland and
Labrador
RN 4 years No data
LPN 16 months High school diploma

74 Journal of Nursing Regulation
TABLE C5 (continued)
Province/Territory Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Nova Scotia RN 3–4 years Grade 12 education with strong science grades
LPN 2 years Completion of Grade 12 education, including Eng
-
lish, mathematics, and two sciences, as well as a
criminal record check, immunizations, and cardio
-
pulmonary resuscitation and first aid certificates
Northwest Territories
and Nunavut
RN 4 years Completion of Grade 12 education, including Eng
-
lish at Grade 12, mathematics at Grade 11, and
two Sciences at a Grade 11 and 12, as well as a
criminal record check
LPN 2 years Completion of Grade 12 education, including Eng
-
lish and science at Grade 12 level, and a criminal
record check
Ontario RN 4 years 12 years of primary and secondary education and
a criminal background check
Registered practical
nurse
2 years 2-year diploma from community college and crim
-
inal background check
Prince Edward Island RN No data No data
LPN 2 years No data
Quebec RN 3 years No data
Saskatchewan RN 4 years Completion of Grade 12 education
RN (additional
authorized practice)
No data Completion of an RN program
LPN No data No data
Yukon RN No data No data
Note. GPA=grade point average; LPN=licensed practical nurse; RN=registered nurse.
TABLE C6
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Specialty
Nurses in Canada
Province/Territory Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Alberta Nurse practitioner 2 years Bachelor’s degree in nursing; criminal record
check; 4,500 hours of RN practice
Psychiatric nurse 2.5 years High school diploma; criminal record check; adult
abuse registry check; and child abuse registry
check
British Columbia Nurse practitioner 2 years Must complete an RN program
Registered psychiat
-
ric nurse
No data No data
Manitoba Nurse practitioner 2 years Bachelor’s degree in nursing and registration or
eligibility for registration as an RN
Registered psychiat
-
ric nurse
4 years High school diploma and satisfactory completion
of a criminal records check in addition to an adult
and child abuse registry checks
New Brunswick Nurse practitioner 2 years Bachelor’s degree in nursing and registration or
eligibility for registration as an RN
Registered psychiat
-
ric nurse
4 years High school diploma, criminal record check, and
adult and child abuse registry checks
Public health nurse Bachelor’s program in nursing, or
a 2-year program in nursing, and a
minimum of 1,125 hours of prac
-
tice in preceding 5 years
Prerequisites that provide a reasonable assurance
of success in the program and the requisite skills
and abilities needed to achieve entry-level
competencies
Clinical nurse
specialist
No data Bachelor’s degree in nursing, RN eligibility
Community health
nurse
Bachelor’s program in nursing, or
2-year program in nursing, and
minimum 1,125 hours of practice
in preceding 5 years
Prerequisites that provide a reasonable assurance
of success in the program and the requisite skills
and abilities needed to achieve entry-level
competencies

www.journalofnursingregulation.com 75Volume 10
•
Special Issue
•
January 2020
TABLE C6 (continued)
Province/Territory Nurse Type Duration of Nursing Program Requirements for Entry Into Program
New Brunswick
(continued)
Private duty nurse Bachelor’s program in nursing, or
2-year program in nursing, and a
minimum of 1,125 hours of prac
-
tice in preceding 5 years
Prerequisites that provide a reasonable assurance
of success in the program, and the requisite skills
and abilities needed to achieve entry-level
competencies
Nova Scotia Nurse practitioner 2 years An RN license and a BScN
Northwest Territories
and Nunavut
Nurse practitioner 2 years Completion of a 4-year undergraduate nursing
program
Ontario Nurse practitioner 1.5–2 years Must hold a BScN in addition to nurse practitioner
diploma or master’s degree; criminal background
check/history in other jurisdictions
Saskatchewan Nurse practitioner No data Must be an active RN with set hours
Registered psychiat
-
ric nurse
3 years Completion of Grade 12 education
Yukon Nurse practitioner No data No data
Note. BScN=bachelor of science degree in nursing; RN=registered nurse.
TABLE C7
Types of Nurses and Nursing Program Requirements for Entry—Caribbean Community
Members
Member State Nurse Type Requirements for Entry Into Program
Bahamas RN Entry into the nursing program is competitive. Nursing student applicant must be a mini
-
mum age of 17 years with satisfaction of education requirements as required by the
Council.
Clinical nurse Entry into the nursing program is competitive. Nursing student applicant must be a mini
-
mum age of 17 years with satisfaction of education requirements as required by the
Council.
Bahamas
(continued)
Midwife Entry into the nursing program is competitive. Nursing student applicant must be a mini-
mum age of 20 years with satisfaction of education requirements as required by the
Council.
Barbados Midwife Associate degree in general nursing or equivalent, along with RN certification
Psychiatric nurse Associate degree in general nursing or equivalent, along with RN certification
Nurse Five passes inclusive of English language and biology at general proficiency level at
Grade 1, 2, or 3 (from June 1998 only); five passes inclusive of English language and biol
-
ogy O Level at Grades A, B or C; or any qualification considered to be equivalent to the
above mentioned.
Auxiliary nurse Must be at least age 17 years
Dominica RN Four GCE or CXC subjects—English and mathematics compulsory
Nurse anesthetist Post-RN training as nurse anesthetist
Nurse assistant Two GCE or CXC subjects
Family nurse practitioner Post-RN training as nurse practitioner
Primary care nurse Two GCE or CXC subjects
Mental health nurse Two GCE or CXC subjects
Granada RN GCE or CXC subjects, which must include mathematics, English language, and a science
subject
Midwife Must be an RN before commencing training in midwifery
Family nurse practitioner Advanced education and training
Community health nurse Training in community nursing
District nurse Must be an RN/midwife with at least 2 years working in a hospital setting
Haiti Pediatric nurse Specialist training for pediatric nurses is open to licensed nurses working in pediatrics.
This training requires entrance exam, curriculum vitae, letter of motivation, diploma and
the state license, reference letter from the supervisor, written test, and interview/ oral ar
-
gumentation with candidate
Jamaica Registered general nurse General proficiency – Grades I, II, III; O Level – Grades A, B or C; CAPE (see below for
CAPE subjects) – Grades 1–4
Applicant shall have studied three compulsory subjects: English language or communi
-
cations studies; science (biology or human and social biology); mathematics, pure math-
ematics, or applied mathematics; and two other subjects from the approved subjects list

76 Journal of Nursing Regulation
TABLE C7 (continued)
Member State Nurse Type Requirements for Entry Into Program
Jamaica
(continued)
Registered midwife Hold an RN license, or:
General proficiency – Grades I, II, III; O Level – Grades A, B or C; CAPE (see below for
CAPE subjects) – Grades 1–4
Applicant shall have studied three compulsory subjects: English language or communi
-
cations studies; science (biology or human and social biology); mathematics, pure math-
ematics, or applied mathematics; and two other subjects from the approved subjects list
Enrolled assistant nurse General proficiency – Grades I, II, III; O Level – Grades A, B or C; CAPE (see below for
CAPE subjects) – Grades 1–4
Applicant shall have studied three compulsory subjects: English language or communi
-
cations studies; science (biology or human and social biology); mathematics, pure math-
ematics, or applied mathematics; and two other subjects from the approved subjects list
Montserrat RN Must be at least age 18 years and have passed at least 2 subjects at the O Level or an
equivalent level, including either English or Natural Science
Registered midwife Must be age 17 years or have the permission of the board to enter and have a Grade B
Seventh Standard Leaving Certificate or its equivalent
Enrolled nursing assistant Must be age 17 years or have the permission of the board to enter and have a Grade B
Seventh Standard Leaving Certificate or its equivalent
Saint Lucia Nurse GCE and CXC qualifications (including either graduation from high school or associate
degree program); passing in 5 main subjects; an interview; and English and mathematics
entrance examination. All student nurses are also required to complete a 2–3 month pre
-
liminary training program.
Saint Vincent
and the
Grenadines
Midwife Be an RN
Trinidad and
Tobago
Midwife Must complete a course of training in a recognized place of training or approved by the
Accreditation Council under the Accreditation Council of Trinidad and Tobago Act and
pass the examination prescribed by the Council or any other nursing examining body
recognized by the Council, and who establishes to the Council’s satisfaction that he or
she is a fit and proper person to be entered on the register as a midwife, shall, on making
an application to the Council and upon compliance with the requirements of this Act, be
entitled to be registered.
A person may be admitted to an approved school of midwifery as a pupil-midwife if the
applicant is registered as a nurse in the Register of Nurses and has passed at least five
subjects at O Level of the GCE, two of the subjects being English language and a subject
that shows proficiency in mathematics. A person shall not be eligible for training as a pu
-
pil-midwife if younger than 21 years or, except at the discretion of the Council, if older
than 50 years.
Nurse A person must complete a training course in a recognized place of training under the
Nursing Personnel Act or under which has been approved by the Council under the Ac
-
creditation Council of Trinidad and Tobago Act and passed the examination prescribed by
the Council or any other nursing examining body recognized by the Council; and who es
-
tablishes to the Council’s satisfaction that he or she is a fit and proper person to be en-
tered on the Register as a nurse.
A person may be admitted to an approved school of nursing as a student nurse if (a) ap
-
plicant is younger than 17 years and not older than 45 years; (b) applicant has passed at
least five subjects at O Level of the GCE, two of the subjects being English language and
a subject that shows proficiency in mathematics
Trinidad and
Tobago
(continued)
Nurse assistant The Council may, in its discretion, authorize the entry on the Roll of Nursing Assistants of
the name of any person who has completed a course of training approved by the Council
and who has passed the examinations prescribed by the Council and who has otherwise
complied with the requirements of the Nursing Personnel Act.
A person must also be of good character; not younger than 18 years and not older than
45 years; and have attained 3 O Level passes with English.
Note. CXC=Caribbean Examinations Council; GCE=General Certificate of Education; O Level=ordinary level; RN=registered nurse.

www.journalofnursingregulation.com 77Volume 10
•
Special Issue
•
January 2020
TABLE C8
Types of Nurses and Duration of Nursing Program and Nursing Program Requirements by
Nurse Type—Caribbean Community Associate Members
Associate
Member State
Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
British Virgin
Islands
Nurse practitioner No data Holds an RN license
Anguilla Advanced practice
nurse
Additional train
-
ing following a
bachelor’s pro
-
gram in nursing
Bachelor’s degree in nursing
RN Bachelor’s pro
-
gram in nursing
Completion of secondary school
Bermuda Advanced practice
nurse
Minimum graduate level
RN 3 years College level entry requirement
Cayman
Islands
RN 4 years High school transcript, certified copy of external examination grades (or if
older than 21 years and without academic qualifications, must have work
experience), and $25 application fee. In lieu of grades, a letter from an em
-
ployer that states the number of years of employment and clearly indicates
its relation to the intended field of study may be submitted.
Turks and
Caicos Islands
RN 4 years Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Turks and
Caicos Islands
(continued)
Nurse practitioner Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Midwife Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Registered nursing
assistant
Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Nurse anesthetist Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Licensed practical
nurse
Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Public health nurse Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Mental health nurse Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Clinical nurse Minimum admission requirements developed and published by the nursing
school, per CARICOM requirements
Note. CARICOM=Caribbean Community; RN=registered nurse.
TABLE C9
Types of Nurses and Duration of Nursing Program and Requirements for Entry by Nurse
Type—Caribbean Community Nonmembers
Caribbean
Nation
Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Aruba Midwife At least 2 years No data
Nurse 3 years High school diploma or equivalent; test of English as foreign
language
Cuba Bachelor of science
in nursing nurse
5 years No data
Specialist nurse No data Nursing graduate
Doctorate of
nursing
3–5 years Nursing graduate
Martinique Midwife 5 years Accessible after the bachelor’s degree; the first year is done at
the university. Admission to a hospital school or to a university
structure dedicated to midwifery training depends on the rank
of the first-year examinations.

78 Journal of Nursing Regulation
TABLE C9 (continued)
Caribbean
Nation
Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Martinique
(contiinued)
Nurse anesthetist 2 years of specialized training
following nurse certification
Must be a state-certified nurse for 2 years, followed by 2 years
of training
Nurse 3 years No data
Operating room
nurse
Initial nursing certification
program followed by 1.5
years of specialized training
Must first be a state-certified nurse for 2 years, then 1.5 years of
specialized training
TABLE C10
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Central
America
Country Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Costa Rica Auxiliary nurse No data No data
Specialist nurse No data No data
Nurse No data No data
El Salvador Bachelor of nursing 5 years 12 years of education
El Salvador
(continued)
Technologist 4 years 12 years of education
Nurse assistant 1 year 12 years of education
Technicians 2 years 12 years of education
Guatemala Professional nurse No data No data
Auxiliary nurse No data No data
Nursing assistant No data No data
Community nursing
assistant
No data No data
Nursing technician No data No data
Bachelor of nursing No data No data
Master’s in nursing No data Completion of a bachelor of nursing degree
PhD nurse No data Completion of a master’s in nursing degree
Honduras Nurse 5 years Intermediate education
Master’s nurse 2 years Licensed in nursing
Nicaragua Registered nurse 3 years Diploma of completion from primary school, and any other re
-
quirements the board of nursing school sees fit
Midwife No data No data
TABLE C11
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Mexico
Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Auxiliary nurse 1.5 years High school
Doctoral nurse 2–3 years Previous study in nursing and master’s degree
General nurse/
nurse technician
3 years and 1 year of social service High school
Licensed nurse 4 years and 1 year of social service High school
Master’s nurse 2–3 years Previous study of nursing degree (license)
Postgraduate
nurse
2–4 years Bachelor’s degree in nursing
Specialist nurse 2 years Bachelor’s degree in nursing
TABLE C12
Types of Nurses and Duration of Nursing Program and Requirements for Entry—General
Nurses in South America
Jurisdiction Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Argentina Nurse 3 years No data
Bolivia Nurse 8 semesters Candidate should be aged 16–20 years, be single, and
have completed at least the third high school year.

www.journalofnursingregulation.com 79Volume 10
•
Special Issue
•
January 2020
TABLE C12 (continued)
Jurisdiction Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Bolivia
(continued)
Graduate nurse 8 semesters Candidate should be aged 16–20 years, be single, and
have completed at least the third high school year.
General nurse 6 semesters Candidate should be aged 16–20 years, be single, and
have completed at least the third high school year.
Chile Nurse Varies by region/municipality, but
duration is 5 years on average for
most nurse training programs
No data
Colombia Undergraduate
nurse/RN
No data No data
Ecuador Nurse Bachelor’s degree, or graduate de
-
gree in nursing
No data
Paraguay Nurse Bachelor’s degree in nursing No data
Peru General nurse University degree program in
nursing
Minimum of high school education (Grade 12)
Uruguay RN Bachelor’s degree program in
nursing
An entrance examination is required. Additionally, candi
-
dates should be morally, mentally, and physically sound
for practice.
Venezuela RN Bachelor’s program in nursing No data
Note. RN=registered nurse.
TABLE C13
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Midwives in
South America
Jurisdiction Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Chile Midwife No data No data
Ecuador Midwife No data No data
Ancestral midwife Midwife training in addition to
“community empowerment”
training
Be a recognized midwife in the community with more than
10 years of experience as a midwife, or a certified midwife
who desires to train to be an ancestral midwife
Peru Midwife Up to 5 years Minimum of high school education (Grade 12)
Uruguay Midwife No data Formal educational training as a nurse
TABLE C14
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Specialist
Nurses in South America
Jurisdiction Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Argentina Licensed nurse 5 years Hold the title of university nurse
Chile Master’s in nursing No data No data
Doctoral nurse No data No data
Colombia Master’s in nursing No data No data
Specialized nurse No data No data
Doctorate in nursing No data No data
Postdoctorate in
nursing
No data No data
Ecuador Advanced practice
nurse
Graduate nursing education after receiving bach
-
elor’s nurse training
Be a certified nurse
Peru Nurse specialist Additional studies beyond nursing studies is
required.
Nursing license

80 Journal of Nursing Regulation
TABLE C15
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Assistant
Nurses in South America
Jurisdiction Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Bolivia Nursing assistant .5 years Candidate should be aged 16–20 years, be single, and have
completed at least the third high school year.
Chile Nursing assistant No data No data
Colombia Auxiliary nurse No data No data
Paraguay Nursing assistant No data No data
Nursing technician No data No data
Peru Nurse assistant No data No data
Uruguay Nursing assistant 2,400 hours Successful completion of first year of high school
TABLE C16
Requirements for Entry Into Nursing Programs by Brazilian State
Brazilian State Nurse Type Requirements for Entry Into Program
Acre Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration, document proving age requirement (16–38 years) is met, and attestations
of physical and mental health, vaccination, and moral suitability
Auxiliary nurse
Nurse technician
Certificate of completion of primary course, official or recognized, certificate of civil reg
-
istration, document proving age requirement (16–38 years) is met, attestations of physi-
cal and mental health and vaccination, and attestation of moral suitability, certificate of
approval in the examination of admission to the first junior year in official or recognized
course, certificate of approval in the entrance examination.
Obstetric Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration, document proving age requirement (16–38 years) is met, and attestations
of physical and mental health, vaccination, and moral suitability
Alagoas Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration, a document proving age requirement (16–38 years) is met, and attestations
of physical and mental health, vaccination, and moral suitability
Obstetric nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration, document proving age requirement (16–38 years) is met, attestations of
physical and mental health, vaccination, and moral suitability
Nursing assistant/
auxiliary nurse
Certificate of completion of primary course, official or recognized, certificate of civil reg
-
istration, document proving age requirement (16–38 years) is met, attestations of physi-
cal and mental health and vaccination, attestation of moral suitability, certificate of ap-
proval in the examination of admission to the first junior year in official or recognized
course, and certificate of approval in the entrance examination
Amapa Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nurse technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration, document proving age requirement (16–38 years) is met, and attestations
of physical and mental health, vaccination, and moral suitability
Nurse assistant Certificate of completion of primary course, official or recognized, certificate of civil reg
-
istration, document proving age requirement (16–38 years) is met.
Amazonas Nurse technician Certificate of completion of primary course, official or recognized, certificate of civil reg
-
istration, document proving age requirement (16–38 years) is met.

www.journalofnursingregulation.com 81Volume 10
•
Special Issue
•
January 2020
TABLE C16 (continued)
Brazilian State Nurse Type Requirements for Entry Into Program
Bahia Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Bahia
(continued) Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nurse technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Ceara Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year, in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nursing technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Distrito Federal Nursing assistant
Nurse technician
Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; certificate of
approval in the entrance examination
Nurse Entrance examination; certificate of completion of secondary course; certificate of civil
registration; document proving age requirement (16–38 years) is met; attestations of
physical and mental health, vaccination, and moral suitability
Espirito Santo Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nursing technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Goias Nursing assistant Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; certificate of
approval in the entrance examination
Nurse Entrance examination; certificate of completion of secondary course; certificate of civil
registration proving age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability
Obstetric nurse Entrance examination; certificate of completion of secondary course; certificate of civil
registration proving age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability
Nurse technician Entrance examination; certificate of completion of secondary course; certificate of civil
registration proving age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability

82 Journal of Nursing Regulation
TABLE C16 (continued)
Brazilian State Nurse Type Requirements for Entry Into Program
Maranhao Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year in official or recognized course; (c) certificate of ap
-
proval in the entrance examination
Maranhao
(continued) Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course
Nursing technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Mato Grosso do Sul Nursing assistant
Nursing technician
Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; and certificate
of approval in the entrance examination
Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration proving the age requirement (16–38 years) is met, and attestations of physi
-
cal and mental health, vaccination, and moral suitability
Obstetric nurse Complete entrance examination; submit certificate of completion of secondary course;
submit certificate of civil registration proving the age requirement (16–38 years) is met;
and submit attestations of physical and mental health, vaccination, and moral
suitability
Minas Gerais Midwife Completion of Grade 12
Nursing assistant Certificate of completion of the primary course, official or recognized; certificate of ap
-
proval in the examination of admission to the first junior year in official or recognized
course; and certificate of approval in the entrance examination
Nurse Certificate of civil registration proving the age requirement (16–38 years) is met; attesta
-
tions of physical and mental health, vaccination, and moral suitability; and certificate of
completion of the secondary course
Para Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nursing technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Paraiba Nursing assistant Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; and certificate
of approval in the entrance examination
Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration proving the age requirement (16–38 years) is met, and attestations of physi
-
cal and mental health, vaccination, and moral suitability
Obstetric nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration proving the age requirement (16–38 years) is met, and attestations of physi
-
cal and mental health, vaccination, and moral suitability.
Nurse technician Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration, proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; and certificate
of approval in the entrance examination

www.journalofnursingregulation.com 83Volume 10
•
Special Issue
•
January 2020
TABLE C16 (continued)
Brazilian State Nurse Type Requirements for Entry Into Program
Parana Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nursing technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Pernambuco Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration proving the age requirement (16–38 years) is met, and attestations of physi
-
cal and mental health, vaccination, and moral suitability
Obstetric nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration, proving the age requirement (16–38 years) is met, and attestations of phys
-
ical and mental health, vaccination, and moral suitability
Nurse technician
Nurse assistant
Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; and certificate
of approval in the entrance examination
Piaui Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For the enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Piaui
(continued) Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nursing technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability
Rio de Janeiro Definitive nursing
assistant
Certificate of civil registration proving age requirement (16–38 years) is met; attesta
-
tions of physical and mental health, vaccination, and moral suitability; entrance
examination.
Applicants will be selected by selection process by the Ministry of Health. Submit one
of the following: certificate of completion of the primary course, official or recognized;
certificate of approval in the examination of admission to the first junior year in official
or recognized course; certificate of approval in the entrance examination.
Definitive nurse Certificate of civil registration proving the age requirement (16–38 years) is met; attesta
-
tions of physical and mental health, vaccination, and moral suitability; certificate of
completion of junior high school; certificate of completion of the secondary course; cer
-
tificate of the commercial course; diploma or certificate of normal course; entrance ex-
amination. Applicants will be selected by selection process by the Ministry of Health.
Rio Grande do Norte Nursing assistant
Nursing technician
Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; certificate of
approval in the entrance examination.
Nurse Entrance examination; certificate of completion of secondary course; certificate of civil
registration proving the age requirement (16–38 years) is met; attestations of physical
and mental health, vaccination, and moral suitability
Obstetric nurse Entrance examination; certificate of completion of secondary course; certificate of civil
registration proving the age requirement (16–38 years) is met; and attestations of physi
-
cal and mental health, vaccination, and moral suitability

84 Journal of Nursing Regulation
TABLE C16 (continued)
Brazilian State Nurse Type Requirements for Entry Into Program
Rio Grande do Sul Nursing assistant Certificate of civil registration proving the age requirement (16–38 years) is met; attesta
-
tions of physical and mental health, vaccination, and moral suitability; entrance exami-
nation. Applicants will be selected by selection process by the Ministry of Health. Appli-
cants will submit one of the following: certificate of completion of the primary course,
official or recognized; certificate of approval in the examination of admission to the first
junior year in official or recognized course; certificate of approval in the entrance
examination.
Nurse Certificate of civil registration proving the age requirement (16–38 years) is met; attesta
-
tions of physical and mental health, vaccination, and moral suitability; certificate of
completion of junior high school; certificate of completion of the secondary course; cer
-
tificate of the commercial course; diploma or certificate of normal course; entrance ex-
amination. Applicants will be selected by selection process by the Ministry of Health.
Rondonia Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For the enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nursing technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Roraiima Nursing assistant
Nurse technician
Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; certificate of
approval in the entrance examination
Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration, proving the age requirement (16–38 years) is met, and attestations of phys
-
ical and mental health, vaccination, and moral suitability
Obstetric nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration proving the age requirement (16–38 years) is met, and attestations of physi
-
cal and mental health, vaccination, and moral suitability
Nursing assistant Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. For enrollment in the nursing assistant
course, one of the following tests shall be required: (a) certificate of completion of the
primary course, official or recognized; (b) certificate of approval in the examination of
admission to the first junior year, in official or recognized course; (c) certificate of ap
-
proval in the entrance examination.
Santa Catarina Nurse Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability. To enroll in the nursing course, completion of
secondary courses is required, and applicants must present one of the following: (a)
certificate of completion of junior high school; (b) certificate of the business course; or
(c) diploma or certificate of normal course.
Nursing technician Applicants must be aged 16–38 years and provide attestations of physical and mental
health, vaccination, and moral suitability.
Sao Paulo Nurse Certificate of civil registration proving the age requirement (16–38 years) is met; attesta
-
tions of physical and mental health, vaccination, and moral suitability; certificate of
completion of junior high school; certificate of completion of the secondary course is
required; certificate of the commercial course; diploma or certificate of normal course;
and satisfactory entrance examination. Applicants will be selected by selection process
by the Ministry of Health.

www.journalofnursingregulation.com 85Volume 10
•
Special Issue
•
January 2020
TABLE C16 (continued)
Brazilian State Nurse Type Requirements for Entry Into Program
Sao Paulo
(continued) Nurse assistant Certificate of civil registration proving the age requirement (16–38 years) is met; attesta-
tions of physical and mental health, vaccinations, and moral suitability; satisfactory en-
trance examination. Applicants will be selected by selection process by the Ministry of
Health. Submit one of the following: certificate of completion of the primary course, of
-
ficial or recognized; certificate of approval in the examination of admission to the first
junior year in official or recognized course; or certificate of approval in the entrance
examination.
Sergipe Nursing assistant
Nursing technician
Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year in official or recognized course; and certificate
of approval in the entrance examination
Nurse Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and attestation of moral suitability; certificate of approval in
the examination of admission to the first junior year, in official or recognized course;
and certificate of approval in the entrance examination
Mental health nurse Entrance examination; certificate of completion of secondary course; certificate of civil
registration proving the age requirement (16–38 years) is met; attestations of physical
and mental health, vaccinations, and moral suitability.
Obstetric nurse Entrance examination; certificate of completion of secondary course; certificate of civil
registration proving the age requirement (16–38 years) is met; attestations of physical
and mental health, vaccination, and moral suitability.
Tocantins Nursing assistant
Nurse technician
Certificate of completion of primary course, official or recognized; certificate of civil reg
-
istration proving the age requirement (16–38 years) is met; attestations of physical and
mental health, vaccination, and moral suitability; certificate of approval in the examina
-
tion of admission to the first junior year; and a certificate of approval in the entrance
examination.
Nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration proving the age requirement (16–38 years) is met, and attestations of physi
-
cal and mental health, vaccination, and moral suitability
Obstetric nurse Entrance examination, certificate of completion of secondary course, certificate of civil
registration proving the age requirement (16–38 years) is met, and attestations of physi
-
cal and mental health, vaccination, and moral suitability.
TABLE C17
Types of Nurses and Duration of Nursing Education by Nurse Type in the United States
Type of Nurse Duration of Education
Licensed practical nurse/licensed vocational nurse Approximately 1 year of vocational program or community college
Registered nurse 2–4 years of education depending on the program. Programs vary from communi
-
ty-type college programs (associate degree, approximately 2 years in length); hos-
pital-based programs (diploma, 3 years in length); college or university programs
(bachelor’s degree, 4 years in length).
Certified nurse practitioner 2–4 years beyond the bachelor’s degree in nursing
Clinical nurse specialist 2–4 years beyond the bachelor’s degree in nursing
Certified nurse anesthetist 2–4 years beyond the bachelor’s degree in nursing
Certified nurse midwife 2–4 years beyond the bachelor’s degree in nursing

86 Journal of Nursing Regulation
Asia
TABLE C18
Types of Nurses and Duration of Nursing Program and Requirements for Entry by Nurse
Type—China and East Asia
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
China Associate nurse 3 years Not available
Bachelor of nursing Not available 4 Years
Doctoral nurse 3 years Not available
Master’s nurse 2–3 years Not available
Midwife 3 years Completion of primary and secondary education
Nurse 3 years Completion of primary and secondary education
Technical nurse 3 years Not available
Hong Kong Children’s nurse 3 years Age 18 years or older and either a Hong Kong School Certificate or equiva
-
lent or satisfactory knowledge, professional experience, or skills
Enrolled nurse 2 years Age 18 years or older and possible educational qualifications, if specified
Psychiatric nurse 2 years Age 18 years or older and possible educational qualifications, if specified
Registered nurse 3 years Age 18 years or older and either a Hong Kong School Certificate or equiva
-
lent or satisfactory knowledge, professional experience, or skills
Registered mental
health nurse
3 years Age 18 years or older and either a Hong Kong School Certificate or equiva
-
lent or satisfactory knowledge, professional experience, or skills
Registered psychiat
-
ric nurse
3 years Age 18 years or older and either a Hong Kong School Certificate or equiva
-
lent or satisfactory knowledge, professional experience, or skills
Macao (Macau) Grade I nurse Not available An applicant must pass an entrance examination.
Nurse graduate Not available An applicant must be a Grade I nurse with 3–4 years of experience or the
equivalent and sufficiently pass a performance evaluation.
Nurse specialist Not available An applicant must have a degree in nursing; have at least 3 years of nursing
practice in a hospital or health center; and sufficiently pass a performance
evaluation.
Graduate nurse
specialist
Not available An applicant must be a specialist nurse with at least 3–4 years of experience
or the equivalent and satisfy a performance evaluation.
Head nurse Not available An applicant must be a graduate nurse specialist or nurse specialist with at
least 3–4 years of related nursing experience and must satisfy a perfor
-
mance evaluation and public discussion of the curriculum.
Nurse supervisor Not available An applicant must be a head nurse with at least 3–4 years of related nursing
experience and must satisfy a performance evaluation and public discus
-
sion of the curriculum.
Japan Nurse specialist Not available An applicant must have a degree in nursing; have at least 3 years of nursing
practice in a hospital or health center; and sufficiently pass a performance
evaluation.
Mongolia Graduate nurse
specialist
Not available An applicant must be a specialist nurse with at least 3–4 years of experience
or the equivalent and must satisfy a performance evaluation.
Head nurse Not available An applicant must be a graduate nurse specialist or nurse specialist with at
least 3–4 years of related nursing experience and must satisfy a perfor
-
mance evaluation and public discussion of the curriculum.
Nurse supervisor Not available An applicant must be a head nurse with at least 3–4 years of related nursing
experience and must satisfy a performance evaluation and public discus
-
sion of the curriculum.
Master’s nurse 2 years Bachelor’s degree
PhD nurse 3 years Master’s degree
North Korea Not available Not available Not available
South Korea Assistant nurse Not available Completion of special secondary or high school education program, or oth
-
er program providing accredited nursing assistant education
Midwife 1 year Completion of all curricula equivalent to elementary and secondary schools
Nurse 3–4 years Completion of all curricula equivalent to elementary and secondary schools
Specialist nurse Not available Not available
Taiwan Nurse practitioner 6 months to 1
year
Not available
Professional regis
-
tered nurse
4–5 years Not available
Registered nurse 3 years Not available

www.journalofnursingregulation.com 87Volume 10
•
Special Issue
•
January 2020
TABLE C19
Duration of Nursing Program and Requirements for Entry by Nurse Type—Central Asia
Jurisdiction Nurse Type Duration of Nursing Program Requirements for Entry Into Program
Afghanistan RN No data No data
Bangladesh RN (6 types) Diploma program: 3 years
Graduate/bachelor’s program:
4 years
Postgraduate program: 2
years
Grade 12 education
Bhutan Bachelor of nursing 4 years or 1-year duration af
-
ter completion and experi-
ence as GNM program
Depending on the program, applicant must pass Grade 12 with
science (physics, chemistry and biology) and/or completed
GNM diploma program
Staff nurse 3 years Completion of Grade 12
Kazakhstan Nurse 3 years 9–11 years of secondary education
Bachelor’s degree
nurse/bachelor’s
nurse
4 years 11 years of secondary education
Kyrgyzstan Nurse/general nurse Bachelor’s program in
nursing
No data
Nepal Nurse 3–4 years depending on
program
Completion of Grade 10
Pakistan Nurse/RN 1–4 years depending on
program
Diploma program: 3 years
Generic BSN: 4 years
Post-RN BSN: 2 years
Fast track post-RN BSN: 1
year
Regarding the diploma program: Age limit of 15–30 years old,
and completion of premedical science with a minimum of 50%
marks in physics, chemistry, and biology as compulsory sub
-
jects; or matric (science) with a minimum of 55% marks in
physics, chemistry, and biology as compulsory subjects
Generic BSN: Age limit of 17–25 years, and premedical science
with a minimum of 50% marks in physics, chemistry, and biolo
-
gy as compulsory subjects
Post-RN BSN: 2 years’ clinical experience with valid Pakistan
Nursing Council registration; matric with science as Higher Ed
-
ucation Commission requirements such as physics, chemistry,
and biology as compulsory subjects
Fast Track Post-RN BSN: 5 years’ clinical experience with valid
Pakistan Nursing Council registration; matric with science as
Higher Education Commission requirements
Sri Lanka RN 2–4 years (depending on if
applicant already completed
general nursing diploma
program)
Completion of high school or work experience as a general
nurse (depending on program)
General nurse 3 years 13 years of formal education
Note. BSN=bachelor of science in nursing; GNM=general nurse midwife; RN=registered nurse.
TABLE C20
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Indian
States and Territories
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Andaman and
Nicobar Islands
(See Tamil Nadu) (See Tamil Nadu) (See Tamil Nadu)
Andhra
Pradesh
RN 3 years, but 4
years if bache
-
lor’s program in
nursing
10 + 2 pass from any recognized board with 40% marks; age 17–35 years by
December 31; and candidates from state open school recognized by a state
government/National Institute of Open School recognized by central
government
Registered midwife 2 years 10 + 2 pass from any recognized board with 40% marks; age 17–35 years by
December 31, candidates from state open school recognized by a state gov
-
ernment or National Institute of Open School recognized by central
government
88 Journal of Nursing Regulation
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Andhra
Pradesh
(continued)
Bachelor of nursing 4 years Minimum age of 17 years on December 31; 10+2 class passed with Science
(PCB) and English core/English elective with aggregate of 45% marks from
recognized board; and medically fit
Post-basic nurse 2–3 years Minimum age, 17 years on December 31; 10 + 2 class passed with science
and English core/English elective with aggregate of 45% marks from recog
-
nized board or other equivalent board; medically fit.
Produce evidence of former training approved by Indian Nursing Council for
a similar duration in any one of the following areas: occupational therapy
techniques; ophthalmic nursing; leprosy nursing; tuberculosis nursing; psy
-
chiatric nursing; neurological and neurosurgical nursing; community health
nursing; cancer nursing; or orthopedic nursing.
Master’s nurse 2 years Holds an RN or RM; medically fit; academic pass of 10 + 2 in prior course
-
work, or 10 + 1 in or before 1986
ANM 2 years 10 + 2 pass from any recognized board with 40% marks, age 17 years by De
-
cember 31; candidates from state open school recognized by a state govern-
ment or National Institute of Open School recognized by central
government
General nurse
midwife
3 years 10 + 2 pass from any recognized board with 40% marks; age 17 years by De
-
cember 31, no older than 35 years; candidates from state open school rec-
ognized by a state government or National Institute of Open School recog-
nized by central government
Arunachal
Pradesh
Bachelor of science
in nursing/basic
nurse
4 years Minimum age, 17 years; 10 + 2 pass in science and English core; 10 + 2 pass;
and medically fit
Health visitor No data No data
ANM 2 years Minimum age, 17 years; 10 + 2 pass preferably with science; 10 + 2 pass
English; 10 + 2 pass; medically fit
General nurse
midwife
3.5 years Minimum age, 17 years, and maximum age, 35 years; 10 + 2 pass preferably
with science, English aggregate; or 10 + 2 in vocational ANM (or equivalent);
or registered ANM; and medically fit
Assam Registered general
nurse
No data No data
Registered general
nurse midwife
No data No data
ANM No data No data
Bihar Bachelor of nursing/
bachelor’s nurse/
basic nurse
4 years Minimum age, 17 years on December 31 of the year in which admission is
sought; medically fit; and academic pass of 10 + 2 in previous coursework
Post-basic nurse 2–3 years Medically fit; holds RN license, or RM license; academic pass of 10 + 2 or
equivalent in previous coursework. Academic pass of 10 +1 in or before
1986 in previous coursework will be accepted; has passed the Higher Sec
-
ondary or Senior Secondary or Intermediate or 10 + 2 or an equivalent ex-
amination recognized by the university for this purpose, and those who
have done 10 + 1 in or before 1986 will be eligible for admission.
Master’s nurse 2 years RN or RM; passing of bachelor of science in nursing (BScN)/BSc honors in
nursing/post-basic BSc nursing with minimum of 55% aggregate marks.
Minimum 1 year of work experience after basic BSc nursing; and minimum
1 year of work experience prior or after post-basic BSc nursing
ANM 2 years Minimum age, 17 years; registered as ANM with State Nursing Registration
Council; medically fit
General nurse
midwife
2.5 years Minimum age, 17 years, and maximum age, 35 years; registered as ANM
with State Nursing Registration Council; medically fit
Chandigarh (See Punjab) (See Punjab) (See Punjab)
Chhattisgarh Bachelor of nursing 4 years 10 + 2 class pass with 45% aggregate
Post-basic nurse 2–3 years 10 + 2 and is a general nurse midwife; or 10+2, is a general nurse midwife
with 2 years of experience

www.journalofnursingregulation.com 89Volume 10
•
Special Issue
•
January 2020
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Chhattisgarh
(continued)
Master’s in nursing 2 years RN and RM of equivalent with any State Nursing Registration Council.
Minimum education requirements passing of: BSc nursing (bachelor of sci
-
ence in nursing)/BSc honors in nursing/post-basic BSc nursing with mini-
mum of 55% aggregate marks.
Candidate should have received BSc nursing/post-basic BSc nursing in an
institution is recognized by Indian Nursing Council. Candidate should have
a minimum of 1 year of work experience after basic BSc nursing and mini
-
mum of 1 year of work experience prior or after post-basic BSc nursing.
ANM 2 years Minimum age of 17 years and education of 10 + 2 class pass
General nurse
midwife
3.5 years Age of 17–35 years; education of 10 + 2 pass
Dadra and
Nagar Haveli
(See Gujarat) (See Gujarat) (See Gujarat)
Daman and Diu (See Gujarat) (See Gujarat) (See Gujarat)
Delhi General nurse
midwife
3.5 years Age of 17–35 years; passing 10 + 2 academics class, with aggregate of 50%;
must be medically fit
Auxiliary nurse 2 years Passing 10 + 2 eligible academic criteria
Post-basic nurse 2–3 years Age of 17–35 years at time of program entry
Goa Nurse 4 years To be eligible to apply for a 4-year nurse program, an applicant should be a
citizen of India; be at least 17 years of age; have passed in any of the general
streams: faculty science, arts and commerce, or vocational; have English as
medium means of instruction; have resided in the state of Goa for a mini
-
mum of 10 years preceding the year of qualifying examination; have studied
and passed XII standard in higher secondary schools of Goa State; and have
passed the Higher Secondary School Certificate (10 + 2) Science Examina
-
tion or its equivalent with a minimum of 50% marks in the aggregate in the
subjects of physics, chemistry, biology, and English
ANM 2 years For ANM program an applicant should be female; be a citizen of India; be
aged 17–35 years; have passed any of the general streams: faculty science,
arts and commerce, or vocational; Course Health Care Science recognized
by equivalent examination with 45% marks in aggregate; be competent with
English; have resided in the state of Goa for a minimum of 10 years preced
-
ing the year of qualifying examination; and have studied and passed XII
standard in higher secondary schools of Goa State
Gujarat Midwife 2–3 years Age, 17–35 years; medically fit. Minimum education: 10 + 2 class passed,
preferably science and English with aggregate of 40% marks; 10 + 2 in arts
(mathematics, biotechnology, economics, political science, history, geogra
-
phy, business studies, accountancy, home science, sociology, psychology,
philosophy) and English core/elective or healthcare science; 10 + 2 vocation
-
al ANM under the board or other equivalent board with 40% marks; regis-
tered as ANM with State Nursing Registration Council.
Nurse 3–4 years Age, 17–35 years; medically fit. Minimum education: 10 + 2 class passed,
preferably science and English with aggregate of 40% marks; 10 + 2 in arts
(mathematics, biotechnology, economics, political science, history, geogra
-
phy, business studies, accountancy, home science, sociology, psychology,
philosophy) and English core/elective or healthcare science.
ANM 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought. Minimum educational requirements shall be 10 + 2 in
arts (mathematics, physics, chemistry, biology, biotechnology, economics,
political science, history, geography, business studies, accountancy, home
science, sociology, psychology, and philosophy) and English core/elective
or science or healthcare science.
Haryana Bachelor of nursing 4 years Minimum age, 17 years; education + 2 with science
Post-basic nurse 2 years Holds a general nurse midwife license
Master’s in nursing 2 years Post-basic BSc nursing, BSc nursing (post-basic bachelor of science in nurs
-
ing; bachelor of science in nursing)
ANM 2 years Minimum age, 17 years; education of + 2 prerequisite
General nurse
midwife
3.5 Age, 17–35 years; education + 2 with science

90 Journal of Nursing Regulation
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Himachal
Pradesh
Midwife 3.5 years Medically fit and age 17–35 years
Nurse 3.5 Age, 17–35 years; must have also attained 10 + 2 in arts and English core/
elective or healthcare science and qualified by examination; be registered
as an ANM with the state nursing registration council; and be medically fit.
Master’s in nursing 2 years Must be an RN and RM; minimum passing of bachelor of science in nursing/
post-basic bachelor of science in nursing (BSc) with minimum of 55% ag
-
gregate marks after completion of designated program; minimum 1 year
work experience after BSc nursing; minimum 1 year work experience prior
to or after post-basic BSc nursing
Health visitor 2 years Not available
ANM 2 years Age 17–35 years on or before December 31 of year in which admission is
sought; must have also attained and qualified in 10 + 2 in arts and English
core/elective, science, or healthcare science educational requirements and
corresponding examination; and must be medically fit.
Basic nurse 4 years Mimimum age of 17 years; 10 + 2 class passed with science and English
core/elective with aggregate of 45% marks from recognized board; medical
-
ly fit; maintain general nursing midwifery degree
Post-basic nurse 2–3 years Passing of the higher secondary, senior secondary, intermediate, 10 + 2 or
equivalent examination; completion of a general nursing and midwifery
program; registration as a RNRM; medically fit
Jammu and
Kashmir
RN/nurse 3–4 years Age, 17–35 years; academic pass of 10 + 2 in prior coursework; medically fit;
entrance examination if entering BSc (N) (bachelor of science in nursing) or
MSc (N) (master of science) in nursing program.
Midwife 2–3.5 years Age, 17–35 years; academic pass of 10 + 2 in prior coursework; medically fit;
entrance examination if entering BSc (N) (bachelor of science in nursing) or
MSc (N) (master of science) in nursing program.
Bachelor of nursing/
bachelor’s nurse
4 years Entrance examination; minimum age, 17 years on December 31 of the year
in which admission is sought; 10 + 2 class passed with science and English
core/English elective with aggregate of 45% marks from recognized board
or other equivalent board; medically fit.
Students appearing in 10 + 2 examination in Science conducted by National
Institute of Open School with 45% marks
Master’s in nursing/
master’s nurse
2 years Entrance examination required; RN or RM; passing education requirements
of BSc (N) (bachelor of science in nursing) or MSc (N) (master of science) in
nursing program of minimum of 55% aggregate marks; should have BSc
nursing / BSc hons. nursing / post-basic BSc nursing.
Minimum 1 year of work experience after basic BSc nursing; minimum 1
year of work experience before or after post-basic BSc nursing
ANM 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought; academic pass of 10 + 2 in arts (mathematics, physics,
chemistry, biology, biotechnology, economics, political science, history, ge
-
ography, business studies, accountancy, home science, sociology, psycholo-
gy, and philosophy) and English core/elective or science or healthcare sci-
ence; medically fit.
Students qualified in 10 + 2 arts or science examination conducted by Na
-
tional Institute of Open School.
Jharkhand Bachelor of nursing/
bachelor’s nurse
4 years Minimum age of 17 years; 10 + 2 academic pass; pass Jharkhand Nursing
Entrance Competitive Examination; medically fit
ANM 2 years Minimum age of 17 years; 10 + 2 academic pass and medically fit
General nurse
midwife
3.5 years Age of 17–35 years; 10 + 2 academic pass with science; medically fit

www.journalofnursingregulation.com 91Volume 10
•
Special Issue
•
January 2020
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Karnataka RN 3 years Age of 17–35 years (women); age 17–30 years (men).
Shall have passed the SSLC or equivalent examinations. Candidates who
have completed, appeared, and failed the SSLC course also shall be consid
-
ered subject to the condition of passing an entrance test that will be con-
ducted by the Board of Examiners for Nurses before they are considered for
selection. The concession is applicable to those who have put in regular at
-
tendance in the last three classes of high school, and appear for SSLC
through high school.
A school leaving certificate showing general educational qualification and
date of birth.
Certificate of Indian nationality.
Registered psychiat
-
ric nurse
Minimum
6-month
program
Passed 3-year general nursing course
RM Minimum of 9
months
Passed 3-year general nursing course
Health visitor 2 years Applicant shall have passed the SSLC or equivalent examinations. Candi
-
dates who have completed, appeared, and failed the SSLC course also shall
be considered subject to the condition of passing an entrance test that will
be conducted by the Board of Examiners for Nurses before they are consid
-
ered for selection. The concession is applicable to those who have put in
regular attendance in the last three classes of high school, and appear for
SSLC through high school. In the case of male candidates, applicant’s age
shall not be less than 17 years or more than 30 years. In the case of female
candidates, applicant’s age shall not be less than 17 years or more than 35
years.
Certificate of Indian nationality.
ANM 2 years Applicant shall produce documentary evidence to prove that applicant is
not younger than 17 years, has passed the first seven classes of schooling,
and is physically fit.
Kerala Midwife 3.5 years 10 + 2 academic pass, based on percentage of marks; medically fit; and
aged at least 17 years but no older than 35 years
Nurse 3.5 years Must be aged at least 17 years but no older than 35 years; must have also
attained 10 + 2 academic pass in arts and English core/elective or healthcare
science and qualified by examination; be registered as an ANM with the
state nursing registration council; and be medically fit.
Master’s in nursing 2 years Must be an RN and RM; minimum passing of bachelor of science in nursing
(BSc [N] /post-basic BSc nursing with minimum of 55% aggregate marks af
-
ter completion of designated program; minimum 1 year work experience af-
ter basic BSc nursing; minimum 1 year work experience prior or after post-
basic BSc nursing
Health visitor 2 years No data
ANM 2 years Age of 17–35 years on or before December 31 of the year in which admis
-
sion is sought; must have attained and qualified in 10 + 2 academic pass in
arts and English core/English elective, science, or healthcare science educa
-
tional requirements and corresponding examination; and must be medically
fit.
Basic nursing 4 years 10 + 2 academic class passed with science and English core/elective with
aggregate of 45% marks from recognized board; medically fit; maintain gen
-
eral nursing midwifery degree; be at least 17 years old
Post-basic nursing 2–3 years Passing of the higher secondary, senior secondary, and intermediate
grades; 10 + 2 academic pass or equivalent examination; completion of a
general nursing and midwifery program; registration as an RN, RM; medi
-
cally fit
PhD in nursing 3–5 years Completion of master of science in nursing and master of philosophy in
nursing programs
Master of philoso
-
phy in nursing
1–2 years Completion of master of science in nursing program

92 Journal of Nursing Regulation
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Madhya
Pradesh
Nurse 3.5 years Age 17–35 years on or before December 31 of the year in which admission
is sought. Additionally, candidates must be medically fit. The minimum edu
-
cational requirements shall be 10 + 2 in arts and English core/English elec-
tive or healthcare science; qualification in 10 + 2 arts or science examination
is also required.
PhD nurse 3–5 years Master of science in nursing degree or master of philosophy in nursing
degree
Bachelor of nursing 4 years Must be at least 17 years old on or before December 31 of the year in which
admission is sought; must be medically fit. The minimum educational re
-
quirements shall be 10 + 2 class passed with science and English core/elec-
tive with a final grade of at least 45%.
Post-basic nurse 2–3 years Must have passed the higher secondary/ senior secondary, intermediate, 10
+ 2, or an equivalent examination recognized by the university for this pur
-
pose. Those who have done 10 + 1 in or before 1986 will be eligible for ad-
mission; must have obtained a certificate in general nursing and midwifery
and registered as an RN/RM with the State Nurses Registration Council and
shall be medically fit.
Master’s in nursing 2 years Bachelor of science (BSc), bachelor of science honors nursing, or post-basic
BSc nursing degree and a corresponding final grade of 55%; 2 years of re
-
lated nursing experience; and registration as a RN or RM with any state
nursing registration council
Licensed health
visitor
2 years Completion of 10 + 2 years of schooling; medically fit
Registered nurse
midwife
3–5 years Age of 17–35 years on or before December 31 of the year in which admis
-
sion is sought; must be medically fit. Minimum educational requirements
shall be 10 + 2 in arts and English core/elective or healthcare science; qualifi
-
cation in 10 + 2 arts or science examination is also required.
ANM 2 years Must be aged at least 17 years old on or before December 31 of the year in
which admission is sought; must be medically fit. Minimum educational re
-
quirements shall be 10 + 2 in arts and English core/elective or science or
healthcare science; qualification in 10 + 2 arts or science examination is also
required.
Maharashtra PhD nurse No data 3–5 years depending on program
Midwife 3 years Age, 17–35 years. 10 + 2 academic pass with English, and must have ob
-
tained a minimum of 40% at the qualifying examination and English individ-
ually from any recognized board. Candidates are also eligible from State
Open School recognized by State Government and National Institute of
Open School recognized by central government. Science is preferable.
Post-basic nurse
(psychiatric nurse,
pediatric nurse, on
-
cological nurse, crit-
ical care nurse)
11 months Passed the higher secondary or senior secondary or intermediate or 10 + 2
or an equivalent examination recognized by the university for this purpose.
Those who have done 10 + 1 in or before 1986, will be eligible for
admission.
Obtained a certificate in general nursing and midwifery and registered as
RN/RM with the State Nurses Registration Council. A male nurse, trained
before the implementation of the new integrated course besides being reg
-
istered as a nurse with State Nurses Registration Council, shall produce evi-
dence of training approved by Indian Nursing Council for a similar duration
in lieu of midwifery in any one of the following areas: occupational therapy
techniques, ophthalmic nursing, leprosy nursing, tuberculosis nursing, psy
-
chiatric nursing, neurological and neurosurgical nursing, community health
nursing, cancer nursing, orthopedic nursing.
Auxiliary nurse 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought. Maximum age, 35 years.
Minimum educational requirements: 10 + 2 in arts (mathematics, physics,
chemistry, biology, biotechnology, economics, political science, history, ge
-
ography, business studies, accountancy, home science, sociology, psycholo-
gy, and philosophy) and English core/elective or science or healthcare
science.

www.journalofnursingregulation.com 93Volume 10
•
Special Issue
•
January 2020
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Maharashtra
(continued)
Master’s in nursing/
master’s nurse
(Master of science
in nursing; master
of philosophy in
nursing)
1–2 years de
-
pending on
program
RN and RM or equivalent with any State Nursing Registration Council.
Minimum education requirements shall be the passing of BSc (bachelor of
science) nursing/BSc hons nursing/post-asic BSc nursing, with minimum of
55% aggregate marks.
Should have received BSc nursing / BSc hons nursing / post-basic BSc nurs
-
ing in an institution recognized by the Indian Nursing Council.
Minimum 1 year of work experience after basic BSc nursing; minimum 1
year of work experience prior or after post-basic BSc nursing.
General nurse
midwife
3 years Age, 17–35 years. 10 + 2 academic pass with English and must have ob
-
tained a minimum of 40% at the qualifying examination and English individ-
ually from any recognized board. Candidates are also eligible from State
Open School recognized by State Government and National Institute of
Open School recognized by the central government. Science is preferable.
Basic nurse/ bache
-
lor of science in
nursing
4 years Minimum age, 17 years on December 31 of the year in which admission is
sought; medically fit.
Minimum education: 10 + 2 class passed with science and English core/elec
-
tive with aggregate of 45% marks from recognized board or other equiva-
lent board.
Students shall qualify in 10 + 2 science examination conducted by National
Institute of Open School with 45% marks. Student shall be admitted once in
a year.
ANM 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought; maximum age, 35 years.
Minimum educational requirements shall be 10 + 2 in arts (mathematics,
physics, chemistry, biology, biotechnology, economics, political science, his
-
tory, geography, business studies, accountancy, home science, sociology,
psychology, and philosophy) and English core/elective or science or health
-
care science — only from recognized board.
Manipur Nurse 2–3 years Minimum age, 17 years, and maximum age, 35 years; 10 + 2 academic pass
is required.
Bachelor of nursing/
bachelor’s nurse
4 years 10 + 2 academic pass or equivalent examination from any recognized board/
university/council with English, physics, chemistry, and biology individually
and securing not less than 50% marks for general and 40% marks for sci
-
ence candidates.
ANM 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought; medically fit.
Minimum educational requirements shall be 10 + 2 academic pass in arts
(mathematics, physics, chemistry, biology, biotechnology, economics, politi
-
cal science, history, geography, business studies, accountancy, home sci-
ence, sociology, psychology, and philosophy) and English core/elective or
science or healthcare science.
General nurse
midwife
3–3.5 years Age, 17–35 years; no age range for ANM and licensed health visitor.
Minimum education requirements: 10 + 2 class academic pass preferably
science and English with aggregate of 40% marks; 10 + 2 pass in arts (Math
-
ematics, biotechnology, economics, political science, history, geography,
business studies, accountancy, home science, sociology, psychology, phi
-
losophy) and English core/elective or healthcare science; 10 + 2 vocational
ANM under board or other equivalent board with 40% marks.
Registered as ANM with State Nursing Registration Council; medically fit.
Health worker 1.5–2 years No data
Meghalaya ANM 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought; medically fit. Minimum educational requirements shall
be 10 + 2 in arts and English core/elective or science or healthcare science.
Qualification in 10 + 2 arts or science examination is also required.
Staff nurse 3–3.5 years Minimum age, 17 years, and maximum age, 35 years, on or before Decem
-
ber 31 of the year in which admission is sought; must be medically fit. Mini-
mum educational requirements shall be 10 + 2 in arts and English core/elec-
tive or healthcare science; qualification in 10+2 arts or science examination
is also required.

94 Journal of Nursing Regulation
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Meghalaya
(continued)
Licensed health
visitor
No data Completion of 10 + 2 years of schooling; medically fit
Mizoram Nurse 3.5 years Age, 17–35 years; medically fit.
Must have also attained 10 + 2 in arts and English core/elective or healthcare
science and qualified by examination.
Must be registered as ANM with the state nursing registration council
ANM 2 years Age of 17–35 years on or before December 31 of the year in which admis
-
sion is sought; medically fit.
Must have also attained and qualified in 10 + 2 in arts and English core/elec
-
tive, science, or healthcare science educational requirements and corre-
sponding examination.
Mizoram
(continued)
Basic nursing 4 years Minimum age, 17 years; medically fit
Must have passed 10 + 2 with science and English core/elective with aggre
-
gate of 45% marks from a recognized board
Nagaland (See Assam) (See Assam) (See Assam)
Odisha (Orissa) Midwife 2–3 years No data
Bachelor of nursing/
bachelor’s nurse/
basic nurse
4 years Minimum age, 17 years on December 31 of the year in which admission is
sought; medically fit.
Minimum education: 10 + 2 academic class passed with science and English
core/elective, with aggregate of 45% marks from a recognized board or oth
-
er equivalent board; 10 + 2 vocational ANM recognized by Indian Nursing
Council with 40% marks.
Student shall succeed in 10 + 2 academic examination in science conducted
by National Institute of Open School with 45% marks.
Post-basic nurse 2 years Hold a license as general nurse midwife; passed the Higher Secondary or
Senior Secondary or Intermediate or 10 + 2 academic or an equivalent ex
-
amination recognized by the university for this purpose.
Those who have done 10 + 1 in or before 1986 are eligible for admission.
Obtained a certificate in general nursing and midwifery and registered as
RN or RM with the State Nurses Registration Council. A male nurse, trained
before the implementation of the new integrated course, besides being reg
-
istered as a nurse with the State Nurses Registration Council, shall produce
evidence of training approved by Indian Nursing Council for a similar dura
-
tion in lieu of midwifery in any one of the following areas: occupational
therapy techniques, ophthalmic nursing, leprosy nursing, tuberculosis nurs
-
ing, psychiatric nursing, neurological and neurosurgical nursing, communi-
ty health nursing, cancer nursing, or orthopedic nursing.
Master’s in nursing 2 years PBBSc (N) (post-basic bachelor of science in nursing) or B.Sc (N) (bachelor
of science in nursing).
RN and RM or equivalent with any State Nursing Registration Council.
Minimum education requirements shall be BSc nursing/BSc hons nursing
(bachelor of science in nursing honors) /post-basic BSc nursing with mini
-
mum of 55% aggregate marks;
Should have received BSc nursing/BSc Hons nursing/post-basic BSc nurs
-
ing in an institution recognized by Indian Nursing Council.
Minimum 1 year of work experience after basic BSc nursing registration;
minimum 1 year of work experience prior or after post-basic BSc nursing.
Health visitor 2–4 years No data
Doctoral nurse 3–5 years M.Sc(N), (Master of Science in Nursing), or master of philosophy in nursing
ANM 2 years Minimum age for admission, 17 years on December 31 of the year in which
admission is sought; medically fit.
Minimum education: 10 + 2 academic class passed with science and English
core/elective, with aggregate of 45% marks from a recognized board or oth
-
er equivalent board; 10 + 2 vocational ANM recognized by Indian Nursing
Council with 40% marks.
Student shall succeed in 10 + 2 academic examination in science conducted
by National Institute of Open School with 45% marks.

www.journalofnursingregulation.com 95Volume 10
•
Special Issue
•
January 2020
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Odisha (Orissa)
(continued)
General nurse
midwife
3 years Minimum age, 17 years on December 31 of the year in which admission is
sought; medically fit.
Minimum education: 10 + 2 academic class passed with science and English
core/English elective, with aggregate of 45% marks from a recognized board
or other equivalent board; 10 + 2 vocational ANM recognized by Indian
Nursing Council with 40% marks.
Student shall succeed in 10 + 2 academic examination in science conducted
by National Institute of Open School with 45% marks.
Pondicherry (See Tamil Nadu) (See Tamil Nadu) (See Tamil Nadu)
Punjab RN 3 years Age, 17–35 years. Education of 10 + 2 academic pass. Should be unmarried,
divorced, or widowed; medically fit.
RM 2 years Evidence of being a qualified nurse; head of applicant’s nursing school certi
-
fies applicant has required clinical experience and attended 75% of formal
instruction. Applicant presents “Case Book” duly completed and signed by
head of school.
Bachelor of nursing 4 years Minimum age, 17 years on December 31 of the year in which admission is
sought; medically fit.
Minimum education: 10 + 2 class passed with science and English core/Eng
-
lish elective with aggregate of 45% marks from recognized board or other
equivalent board; will have passed 10 + 2 examination in science conducted
by National Institute of Open School with 45% marks.
Master’s in nursing 2 years RN and RM or equivalent with any State Nursing Registration Council.
Minimum education requirements shall be the passing of bachelor of sci
-
ence in nursing/bachelor of science in nursing honors (BSc nursing / BSc
hons. nursing) / post-basic BSc nursing with minimum of 55% aggregate
marks.
Minimum 1 year of work experience after basic BSc nursing; minimum 1
year of work experience prior or after post-basic BSc nursing.
ANM 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought; medically fit.
Minimum educational requirements shall be 10 + 2 academic pass in arts
(mathematics, physics, chemistry, biology, biotechnology, economics, politi
-
cal science, history, geography, business studies, accountancy, home sci-
ence, sociology, psychology, and philosophy) and English core/elective or
science or healthcare science.
Student passed 10 + 2 in arts or science examination conducted by National
Institute of Open School.
General nurse
midwife
3.5 years Minimum age, 17 years, and maximum, 35 years. No age limit for ANM or
lady health visitor; medically fit.
Minimum education: 10 + 2 class passed, preferably science and English
with aggregate of 40% marks; 10 + 2 in arts (mathematics, biotechnology,
economics, political science, history, geography, business studies, accoun
-
tancy, home science, sociology, psychology, philosophy) and English core/
elective or healthcare science from a recognized board or other equivalent
board with 40% marks; 10 + 2 vocational ANM under the board or other
equivalent board with 40% marks.
Registered as ANM with State Nursing Registration Council.
Qualified in 10 + 2 arts or science examination or healthcare science con
-
ducted by National Institute of Open School with 40% marks.
Multipurpose health
worker
2 years Matriculate education criteria

96 Journal of Nursing Regulation
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Rajasthan Midwife 3.5 years Minimum age, 17 years, and maximum, 35 years; 10 + 2 academic pass
based on a percentage of marks; and medically fit
Nurse 3–3.5 years 10 + 2 academic pass based on percentage of marks medically fit, and aged
17–35 years
Master’s in nursing 2 years RN and RM
Minimum passing of bachelor of science in nursing and bachelor of science
honors nursing, or post-basic bachelor of science (BSc nursing/BSc hons.
nursing/post-basic BSc) in nursing with minimum of 55% aggregate marks
after completion of designated program.
Minimum 1-year work experience after basic BSc nursing; minimum 1 year
work experience prior or after post-basic BSc nursing
Health visitor 2 years Not available
ANM 2 years Age, 17–35 years; 10 + 2 academic pass based on percentage of marks;
medically fit
Rajasthan
(continued)
Basic nursing/basic
nurse
4 years Minimum age, 17 years; medically fit; 10 + 2 class passed with science and
English core/elective with aggregate of 45% marks from recognized board;
maintain general nursing midwifery degree
Post-basic nursing/
Post-basic nurse
2–3 years RN or RM; passing of the higher secondary, senior secondary, or intermedi
-
ate education; 10 + 2 academic pass or equivalent examination; completion
of a general nursing and midwifery program; medically fit
Sikkim (See West Bengal) (See West
Bengal)
(See West Bengal)
Tamil Nadu Registered nurse
midwife
3–4 years, de
-
pending on the
program
No data
Tamil Nadu
(continued)
ANM 2 years Minimum age, 17 years, and maximum, 35 years; medically fit. Must attain
10 + 2 in arts (math, physics, chemistry, biology, biotechnology, economics,
political science, history, geography, business studies, accountancy, home
science, sociology, psychology, philosophy) and English core/elective or sci
-
ence or healthcare science from a recognized board.
Telangana (See Andhra
Pradesh)
(See Andhra
Pradesh)
(See Andhra Pradesh)
Tripura Midwife 3.5 years Minimum age, 17 years, and maximum, 35 years, on or before December 31
of the year in which admission is sought; medically fit. Minimum education
-
al requirements, 10 + 2 in arts and English core/elective or healthcare sci-
ence; qualification in 10 + 2 arts or science examination also required.
Health visitor 2 years (18
months and
6-month
internship)
10 + 2 years of schooling
General nurse 3.5 years Minimum age, 17 years, and maximum, 35 years, on or before December 31
of the year in which admission is sought; medically fit. Minimum education
-
al requirements, 10 + 2 in arts and English core/elective or healthcare sci-
ence; qualification in 10+2 arts or science examination also required.
ANM 2 years Minimum age, 17 years on or before December 31 of year in which admis
-
sion is sought; medically fit. Minimum educational requirements, 10 + 2 in
arts and English core/elective or science or healthcare science; qualification
in 10 + 2 arts or science examination also required.
Multipurpose
supervisor
No data No data
Multipurpose work
-
er (health)
No data No data
Uttar Pradesh Midwife 2–3 years Minimum age, 17 years; medically fit; 10 + 2 academic pass
Bachelor of nursing/
bachelor’s nurse
4 years Minimum age, 17 years on December 31 of the year in which admission is
sought; medically fit. Minimum education requirements: 10 + 2 class passed
with science and English core/elective with aggregate of 45% marks from
recognized board or other equivalent Board. 10 + 2 examination in science
conducted by National Institute of Open School with 45% marks.

www.journalofnursingregulation.com 97Volume 10
•
Special Issue
•
January 2020
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Uttar Pradesh
(continued)
Mental health
nurse/post-basic di
-
ploma in psychiatric
nursing
2–3 years RN or RM; medically fit; passed the Higher Secondary, Senior Secondary, or
Intermediate or 10 + 2 or equivalent examination. Those who have done 10 +
1 in or before 1986 are eligible for admission.
Master’s in nursing/
master’s nurse
2 years RN or RM or equivalent with any State Nursing Registration Council. Mini
-
mum education requirements: passing of BSN/BSN honors/post-basic BSN
with minimum of 55% aggregate marks. Candidate should have undergone
BSN/BSN honors/post-basic BSN and have 1 year (minimum) of work expe
-
rience after basic BSN degree completion & 1 year (minimum) of work ex-
perience before or after post-basic BSN degree completion.
General nurse 3 years Minimum age, 17 years, and maximum, 35 years; medically fit; attain aca
-
demic passing score of 10 + 2
ANM 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought; medically fit.
Minimum educational requirements: 10 + 2 in arts (mathematics, physics,
chemistry, biology, biotechnology, economics, political science, history, ge
-
ography, business studies, accountancy, home science, sociology, psycholo-
gy, and philosophy) and English core/elective or science or healthcare sci-
ence — from recognized Board.
Students qualified in 10 + 2 arts or science examination conducted by Na
-
tional Institute of Open School.
General nurse
midwife
3 years Minimum age, 17 years, and maximum, 35 years.
Minimum education requirements: 10 + 2 class passed preferably Science &
English with aggregate of 40% marks. 10 + 2 in arts (mathematics, biotech
-
nology, economics, political science, history, geography, business studies,
accountancy, home science, sociology, psychology, philosophy) and English
core/elective or healthcare science with 40% marks; 10 + 2 vocational ANM
under recognized board or other equivalent board with 40% marks.
Must be registered as ANM with State Nursing Registration Council.
Post-basic nursing/
post-basic nurse
2–3 years Must have passed the Higher Secondary, Senior Secondary, Intermediate,
10 + 2, or equivalent examination recognized by the university for this pur
-
pose. Those who have done 10 + 1 in or before 1986 will be eligible for ad-
mission. Must be medically fit and have obtained a certificate in general
nursing and midwifery and registered as an RN/RM with the State Nurses
Registration Council. A male nurse, trained before the implementation of
the newly integrated course besides being registered as a nurse with the
State Nurses Registration Council, shall produce evidence of training ap
-
proved by Indian Nursing Council for a similar duration in lieu of midwifery
in any one of the following areas: ophthalmic nursing, leprosy nursing, psy
-
chiatric nursing, neurological and neurosurgical nursing, community health
nursing, cancer nursing, orthopedic nursing.
Health worker
(female)
2 years Minimum age, 17 years; medically fit
Uttarakhand Bachelor of nursing/
Bachelor’s nurse/ba
-
sic nurse
4 years Entrance examination; minimum age, 17 years on December 31 of the year
in which admission is sought; medically fit. 10 + 2 class passed with science
and English core/English elective with aggregate of 45% marks from recog-
nized board or other equivalent board
ANM 2 years Minimum age, 17 years on or before December 31 of the year in which ad
-
mission is sought; medically fit. Applicants must attain a passing score of 10
+ 2 in arts (mathematics, physics, chemistry, biology, biotechnology, eco
-
nomics, political science, history, geography, business studies, accountancy,
home science, sociology, psychology, and philosophy) and English core/
elective or science or healthcare science—from recognized board.

98 Journal of Nursing Regulation
TABLE C20 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Uttarakhand
(continued)
Post-basic nurse 2–3 years Applicant must have passed the Higher Secondary, Senior Secondary or In-
termediate examination with a score of 10 + 2 or an equivalent examination
(10 + 1 in or before 1986 will be eligible); medically fit.
If a male nurse, must have been trained before the implementation of the
new integrated course besides being registered as a nurse with the State
Nurses Registration Council and shall produce evidence of training ap
-
proved by Indian Nursing Council for a similar duration in lieu of midwifery
in any one of the following areas: ophthalmic nursing, leprosy nursing, psy
-
chiatric nursing, neurological and neurosurgical nursing, community health
nursing, cancer nursing, orthopedic nursing.
Master’s in nursing/
master’s nurse
2 years Entrance examination; RN or RM status; passing education requirements of
BSN/BSN honors/post-basic BSN with minimum of 55% aggregate marks.
Applicant should have BSN/BSN Honors/post-basic BSN and a minimum of
1 year of work experience after basic BSN and a minimum of 1 year of work
experience prior or after post-basic BSN.
General nurse
midwife
2–3 years Minimum age, 17 years, and maximum, 35 years; medically fit.
Academic passing score of 10 + 2 in prior courses and English with aggre
-
gate of 40% marks is required. 10 + 2 in arts (mathematics, biotechnology,
economics, political science, history, geography, business studies, accoun
-
tancy, home science, sociology, psychology, philosophy) and English core/
elective or healthcare science —from recognized board or other equivalent
board with 40% marks is also required, with 10 + 2 vocational ANM under
recognized board or other equivalent board with 40% marks.
Must be registered as ANM with State Nursing Registration Council.
West Bengal Midwife 3 years 10 + 2 based on grade percentage of marks
Nurse 3 years 10+2 based on grade percentage of marks
Master’s in nursing 2 years Completion of BSN and post-basic BSN programs
ANM 2 years 10 + 2 based on grade percentage of marks
Basic nursing/basic
nurse
4 years 10 + 2 of grade percentage marks and a minimum of 50% in aggregate
Post-basic nursing/
post-basic nurse
1–2 years, de
-
pending on
program
Diploma in general nursing midwifery
Note. ANM=auxiliary nurse midwife; BSN=bachelor of science in nursing; RM=registered midwife; RN=registered nurse; SSLC=Secondary School
Leaving Certificate.
TABLE C21
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Midwives in
Central Asia
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Afghanistan Assistant midwife No data Must pass an Afghan National Testing and Certification Midwifery
Examination
Kyrgyzstan Midwife 3 years Minimum high school education, Grade 10
Nepal Midwife 3 years Completion of Grade 10
Pakistan Nurse midwife 1 year Must be a registered nurse
Community
midwife
1.5 years Age limit between 15 and 40 years; 40% marks in matric (either art or
science)
Sri Lanka Midwife No data No data
Uzbekistan Midwife 3 years Completion of Grade 12
Nurse midwife No data No data

www.journalofnursingregulation.com 99Volume 10
•
Special Issue
•
January 2020
TABLE C22
Duration of Nursing Program and Requirements for Entry—Specialist Nurses in Central Asia
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Afghanistan Nurse anesthetist 2 years following
education for
nurse
No data
Bhutan Master’s in nursing 1 year Completion of bachelor of science in nursing program
Kyrgyzstan Nurse Specialist 1–2 additional
years following
completion of
nursing program
Bachelor’s in nursing or RN
Pakistan Licensed practical
nurse
2 years Program is for females only, age between 15 and 30 years.
Premedical science with a minimum of 45% marks in physics, chemistry,
and biology as compulsory subjects; or matric (science) with a minimum of
45 % marks in physics, chemistry, and biology as compulsory subjects
Lady health visitor 2 years Program is for females only, age between 15 and 30 years.
Premedical science with a minimum of 45% marks in physics, chemistry and
biology as compulsory subjects; or matric (science) with a minimum of 45%
marks in physics, chemistry and biology as compulsory subjects
TABLE C23
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Nurses in
Southeast Asia
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Brunei RN No data No data
Cambodia Associate degree
nurse
3 years Completion of high school education
Bachelor of science
in nursing
4 years Completion of high school education
Indonesia Nurse 3–4 years No data
Laos RN/associate nurse/
high-level nurse
3 years Applicant must have completed an upper secondary school program and
passed an entrance examination.
Graduate nurse/
bachelor-level nurse
2 years (continu
-
ing education
program) or 4
years (direct en
-
try program)
If completing a direct entry program, an applicant must have completed an
upper secondary school program and passed an entrance examination to
the graduate nursing program.
If completing a graduate nursing program by continuing education, an ap
-
plicant must be younger than 45 years and have more than 3 years of expe-
rience as an RN.
Technical nurse/
middle-level nurse
2.5 years Applicant must have completed an upper secondary education program
and passed an entrance examination.
Malaysia Nurse 3 years No data
Myanmar RN 3–4 years, de
-
pending on di-
ploma or degree
program
Completion of high school education (Grade 12)
Nurse midwife 3–4 years, de
-
pending on di-
ploma or degree
program
Completion of high school education (Grade 12) and entrance requirements
as established by the Myanmar Nurse and Midwife Council
Philippines Professional nurse 3 years No data
Singapore RN 3–4 years For the bachelor program, applicants must have attained “A” level in GCE
courses; for the diploma program, applicants must have attained O Level in
GCE courses, including in English, mathematics, and science.
Enrolled nurse 2 years For O Level, any 2 subjects (grade 1–8); for N Level, 3 subjects to include
English, mathematics, and one other subject (Grades 1–5)

100 Journal of Nursing Regulation
TABLE C23 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Thailand Professional nurse 4 years Completion of 12 years of primary and secondary education; minimum age,
16 years; possesses no prohibited disease as prescribed by the Nursing
Council; has not declared bankruptcy/has not been bankrupt; and has not
been declared incompetent, quasi-incompetent, or insane
Vietnam Nurse 4 years Completion of 12 years of basic education, or if already a secondary nurse/
midwife, at least 5 years of experience, is required. Also, must possess a
foreign language level A or a minor ethnic language as well as a basic level
in informatics/computer software data analysis
Elementary nurse 1 year Completion of 9 years of basic education
Secondary nurse 2 years Completion of 12 years of basic education
Vietnam
(continued)
College nurse 3 years Completion of 12 years of basic education; foreign language level A or a mi-
nor ethnic language; and a basic level of computer and software application
Advanced nurse 2 years Completion of a bachelor of science in nursing degree and have worked as
a nurse for at least 9 years; proficiency in computer software related to
monitoring and caring for patients; and must possess a foreign language
level B or fluently use a minor ethnic language
Note. GCE=General Certificate of Education; O Level=ordinary level; RN=registered nurse.
Australia and Oceania
TABLE C24
Types and Duration of Nursing Program and Requirements for Entry—General Nurses in
Australia and Oceania
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Australia RN 3 years No data
Enrolled nurse 1.5 years No data
Cook Islands RN 3 years Minimum age, 17 years; preferred academic criteria; Level 2 with pass in
English; pass Level 1 mathematics and a science subject; two supportive
references.
Men and women older than 21 years: fluent in English; show ability to cope
with an academic course (preferably some recent education)
Fiji RN 3 years No data
Kiribati RN 3 years Form 6 and 7 (science students) test and interview
Enrolled nurse 3 years Form 6 and 7 (science students) test and interview
Marshall
Islands
RN No data Completion of high school
LPN No data No data
Graduate nurse No data Completion of high school
Graduate practical
nurse
No data Completion of high school
Micronesia RN No data No data
LPN No data No data
Nauru RN 3–4 years Completion of Grade 12 and requisite science subjects
New Zealand RN 3 years University entrance or equivalent
Enrolled nurse 1.5 years 3 years of secondary schooling
Palau RN No data Must be physically and mentally fit
LPN No data Must be physically and mentally fit
Papua New
Guinea
RN 3–4 years Required for entry into the 3-year diploma program in nursing: Completion
of Grade 12, and a minimum of C grade average in English, language/litera
-
ture, mathematics, biology, and one or two other major subjects
Required for entry in the 4-year diploma program in nursing: minimum B
grade average in English, mathematics, biology, science (chemistry and/or
physics)
Samoa RN 3 years Foundation year or mature entry
Enrolled nurse 2 years Foundation year or mature entry
Solomon
Islands
RN 3–4 years Secondary form 6/7 (science) with passes in English, mathematics, and sci
-
ence, or passed tests set by the institution

www.journalofnursingregulation.com 101Volume 10
•
Special Issue
•
January 2020
TABLE C24 (continued)
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Tonga RN 3 years No data
Tuvalu RN 3 years Form 7
Vanuatu RN 3 years Must be aged between 18 and 30 years and must have attained 12/13 certifi
-
cate with good grades in science
Note. LPN = licensed practical nurse; RN=registered nurse.
TABLE C25
Types of Nurses and Duration of Nursing Programs and Requirements for Entry—Midwives
in Oceania
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Cook Islands Registered midwife No data No data
Fiji Midwife No data No data
Kiribati Midwife 7–8 months, plus
additional
3-month
internship
Must be an RN or medical assistant
Marshall
Islands
Certified nurse
midwife
No data Completion of high school
Micronesia Nurse midwife No data No data
Nauru Midwife 1 year Diploma of nursing
Palau Certified nurse
midwife
No data Must be physically and mentally fit, shall submit to physical or mental eval
-
uation if requested by Board of Health Professions
Papua New
Guinea
Registered midwife 1–1.5 years Must be an RN and have 2 years’ minimum postregistration experience be
-
fore applying to a midwifery program
Samoa Registered midwife 1 year Must have bachelor of nursing degree
Tonga Midwife 1 year Completion of RN program
Tuvalu Registered midwife 1 year Must be an RN with at least 5 years of experience
Vanuatu Midwife 9 months Must be an RN with more than 5 years of clinical experience
Note. RN=registered nurse.
TABLE C26
Types of Nurses and Duration of Nursing Programs and Requirements for Entry—Specialty
Nurses in Australia and Oceania
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Australia Nurse practitioner 1.5 years No data
Cook Islands Nurse practitioner No data Must hold an RN license
Public health nurse 3 years Minimum age, 17 years preferred academic criteria: Level 2 with pass in
English, pass in Level 1 mathematics and a science subject; two supportive
references.
Males and females older than 21 years: enthusiastic about nursing with
characteristics suitable for nursing; have work experience that shows ability
to work effectively with people; at least two supportive references; fluent in
English (speaking, reading, and writing); show ability to cope with an aca
-
demic course (preferably some recent education).
Mental health nurse 3 years See Cook Islands, public health nurse
Community nurse 3 years See Cook Islands, public health nurse
Fiji Nurse practitioner No data No data
Nurse specialist No data No data
Public health nurse No data No data
Kiribati Public health nurse 5–6 months Must be an RN or medical assistant
Medical assistant 1.5 years Must be an RN with 5 years of work experience in public health

102 Journal of Nursing Regulation
TABLE C26 (continued)
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Marshall
Islands
Nurse practitioner No data Must be an RN
Advanced nurse
Practitioner
No data Must be an RN
Micronesia Nurse practitioner No data No data
Advanced practice
nurse
No data No data
Nurse anesthetist No data No data
Nauru Nurse practitioner No data No data
Nurse specialist No data No data
Nurse anesthetist No data No data
New Zealand Nurse practitioner 2 years Must be an RN with 5 years of work experience
RN prescriber in pri
-
mary health and
specialty teams
1 year Postgraduate diploma
RN prescriber in
community health
6 months–1 year No data
Palau Advanced
practice7nurse
No data Must be an RN
Certified nurse
anesthetist
No data Must be an RN
Papua New
Guinea
Registered mental
health nurse
No data Must be an RN
Registered nurse
practitioner
No data Must be an RN
Registered pediatric
nurse
No data Must be an RN
Registered acute
nurse
No data Must be an RN
Samoa Nurse consultant
specialist
No data No data
Solomon
Islands
Nurse specialist 1 year Must be an RN
Tonga Nurse practitioner No data No data
Tuvalu Nurse practitioner 1 year Must be an RN and midwife
Vanuatu Nurse practitioner 9 months Must be an RN with more than 5 years of clinical experience
Advanced nurse
practitioner
9 months Must be an RN with more than 5 years of clinical experience
Note. RN=registered nurse.
TABLE C27
Types of Nurses and Duration of Nursing Programs and Requirements for Entry—Nurse
Assistants in Oceania
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Cook Islands Nurse aid No data No data
Kiribati Nurse aid No data No data
Marshall
Islands
Nurse assistant No data No data
Operating room
technician
No data No data
Palau Health assistant No data Must be physically and mentally fit, shall submit to physical or mental eval
-
uation if requested by the Board of Health Professions
Papua New
Guinea
Nurse aid/enrolled
nurse
No data No data
Solomon
Islands
Registered nurse
aid
1.5 years Secondary form 3, or tests passed as set by the institution

www.journalofnursingregulation.com 103Volume 10
•
Special Issue
•
January 2020
TABLE C27 (continued)
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Vanuatu Nurse aid 9 months Must have Year 10 certificate with experience as a village health worker or
nurse aid in a hospital/health center setting
Village health
worker
11 weeks Must have Year 6 or 10 certificate; chosen by the community
Europe
TABLE C28
Types of Nurses and Duration of Nursing Program and Requirements for Entry by Nurse
Type—Eastern Europe
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Albania Registered nurse 3–5 years Set by nursing faculty
Belarus Nurse (medical
sister)
No data No data
Midwife No data No data
Bosnia and
Herzegovina
Medical nurse
(nurse)
No data Completion of high school education
Medical midwives
sisters (midwife)
No data Completion of high school education
Health worker No data Completion of high school education
Pediatric nurse (pe
-
diatric nurse sister)
No data Completion of high school education
Psychiatric nurse
sister
No data Completion of high school education
Nursing technician No data High school education in nursing profession
Nurse specialist No data Holds a license in nursing or midwifery
Bulgaria Nurse 4 years Completion of 10 years’ general education with diploma or similar certifica
-
tion, issued by competent body
Midwife 3 years Completion of 10 years’ general education with diploma or similar certifica
-
tion issued by competent body; or evidence of formal qualifications as a
nurse
Health assistant No data No data
Croatia General care nurse 3 years 10 years of general educational program
Bachelor of nursing 3 years 12 years of general educational program
Cyprus General nurse/nurse
technician
3 years Completion of 12 years of general schooling, which provides access to a
university or a higher education institution at a level as equivalent; or com
-
pletion of general school education of at least 10 years, which provides ac-
cess to a vocational school or professional nursing program is required. Ad-
ditionally, applicant should be at least 21 years old and a resident of Cyprus.
Midwife 1.5–3 years, de
-
pending on the
program
Completion of at least 12 years of general school education or possession of
a certificate confirming the success of an entrance examination, equivalent
level in Professional Class I obstetrics or possession of evidence of formal
qualifications as a nurse responsible
Psychiatric nurse No data No data
Health visitor No data No data
Estonia Registered nurse 3.5 years High school graduation certificate
Nurse specialist 0.5–1 year Must be a registered nurse
Advanced nurse
practitioner
2 years Must be a registered nurse
Greece Nurse 4 years 12 years of basic education; entry after national examinations
Nurse assistant 2 years 10 years of basic education; entry without examination
Latvia Nurse 3–4 years No data
Midwife 3 years Completion of secondary education that provides rights to study at a uni
-
versity type higher education institution or education of a nurse

104 Journal of Nursing Regulation
TABLE C28 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Lithuania Nurse general
practitioner
3.5 years Secondary education is required to enter studies.
Nurse general prac
-
titioner and
professional
2 years master’s
degree program
To enter studies: acquire bachelor’s degree in nursing and professional
qualification of nurse general practitioner
Macedonia,
Former Yugo
-
slav Republic
Nurse No data University degree
Midwife No data No data
Republic of
Moldova
Nurse No data No data
Medical assistant No data No data
Montenegro Nurse No data No data
Romania Nurse (assistant
medical generalist)
No data 12 years of education (high school)
Russia Nurse 2 years and 10
months
9–11 years of education
Feldsher 3 years and 10
months
11 years of education
Serbia Professional nurse No data No data
Specialist profes
-
sional nurse
No data No data
Expert Nurse No data No data
Turkey Specialized nurse Varies Varies
Nurse 4 years Completion of higher secondary education
Midwife No data No data
Ukraine Nurse 3 years Completion of secondary education and successful passing of an interview
with board are required.
Midwife No data Completion of secondary education and successful passing of an interview
with board
Specialist nurse No data No data
TABLE C29
Types of Nurses and Duration of Nursing Program and Requirements for Entry—General
Nurses in Nordic Countries
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Norway General nurse 3 years Completion of 10 years of general education
Sweden Nurse 3 years Successful completion of a high school education; proficiency in English
and Swedish
Denmark Nurse 3.5–4 years Completion of 10 years of general education
Finland Nurse 3.5 years Completion of secondary school or equivalent
Iceland Nurse 4 years Completion of secondary school or equivalent
Faroe Islands Nurse No data No data
Greenland Nurse 3 years Greenland permanent residency; completion of secondary school education
and satisfactory passing of an entrance examination
TABLE C30
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Midwives in
Nordic Countries
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Norway Midwife 2 years No data
Sweden Midwife 1.5 years A completed bachelor’s degree in any major in the health sciences or the
equivalent; 1 year’s professional experience as a nurse at the beginning of
the course and language skills equivalent to Swedish B and English A
Denmark Midwife 1.5–3.5 years Completion of high school education
Finland Midwife 1 year Completion of registered nursing program or equivalent

www.journalofnursingregulation.com 105Volume 10
•
Special Issue
•
January 2020
TABLE C30 (continued)
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Faroe Islands Midwife No data No data
Greenland Midwife 3 years Greenland permanent residency; completion of secondary school education
and satisfactory passing of an entrance examination
TABLE C31
Types of Nurses and Duration of Nursing Program and Requirements for Entry in Denmark
Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Psychiatric nurse 1 year Danish authorization as a nurse; 2 years of work experience in clinical psychiat
-
ric nursing and 1-year agreement with employer regarding participation in the-
ory education and guided clinical education
Nurse anesthetist 2 years Danish authorization as a nurse; 2 years of work experience at the broad clini
-
cal level
Health visitor 1.5 years Danish authorization as a nurse; 2 years of work experience at the clinical level,
including completion of 8-month (minimum) appointment in specialized care
and 6-month agreement with employer regarding participation in guided clini
-
cal education
Intensive care nurse 1.5 years Danish authorization as a nurse; 2 years of work experience at the clinical level
and completion of 6-month appointment in intensive care department
Cancer care nurse 1.5 years Danish authorization as a nurse; 2 years of work experience at the clinical level
Hygiene nurse 30 weeks Danish authorization as a nurse; 2–3 years in clinical nursing and at least 1 year
of higher education in nursing after completing general nursing education
TABLE C32
Types of Nurses and Duration of Nursing Program and Requirement for Entry—General
Nurses in Western/Central Europe
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Andorra General nurse 4 years State diploma in secondary education or equivalent
Austria Nurse 3 years Medical fitness; trustworthiness; successful completion of 10 school grades;
admission test or interview whereby a board decides on admission
Belgium General care nurse 4 years Completion of 12 years of general education
Czech Republic GeneralnNurse No data General education of 10 years as attested to by diploma/ certificate or
equivalency
France Nurse 3 years Bachelor’s degree prior to admission into nursing education
Germany Nurse 3 years Proof of middle school and secondary diploma or another equivalently rec
-
ognized degree; successfully completed vocational training of at least 2
years; or, regulated assistance or helper training in care of at least 1 year; or,
permission as a medical assistant; or at least 1 year duration as geriatric
nursing assistant; or licensed as a nursing assistant.
There is a minimum age requirement; some schools set maximum age re
-
quirements, though a maximum age is not required by law.
Hungary General nurse 3 years Completion of secondary school
Bachelor of nursing 4 years No data
Master’s in nursing 1.5 years Completion of bachelor of science in nursing degree
Graduate nurse No data No data
Ireland General nurse 4 years Standard applicants must have a Leaving Certificate and examination mini
-
mum grade of H5 in two higher level papers, and O6/H7 in four ordinary or
higher level papers in the following subjects: Irish or English, mathematics,
a laboratory science subject, and three other subjects. Otherwise, they must
be judged by the higher education institutions to have attained equivalent
minimum education.
Italy RN—general 3 years Completion of secondary school
RN—pediatric 3 years Completion of secondary school

106 Journal of Nursing Regulation
TABLE C32 (continued)
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Liechtenstein Nurse 3 years Completed basic education in accordance with the provisions of regulations
in a recognized institution or an outside regulated program, or, has acquired
experience of at least 3 years of professional experience in the health field
Luxembourg Nurse 4 years Completion of general education of 10 years or equivalent
Malta RN 3 years Completion of 10 years of general education with diploma or similar
certification
Enrolled nurse No data Completion of 10 years of general education with diploma or similar
certification
Monaco Licensed nurse 3 years Must be at least 17 years old on December 31 of year of selection tests; be
mentally and physically fit with attestations of health and character; suc
-
cessfully pass a selection test; and submit documents indicating general2e-
ducation attained
Netherlands Nurse No data No data
Poland RN 2–5 years Completion of primary school
Nurse with bache
-
lor’s degree in
nursing
3 years Completion of high school and passing of matriculation examination
Nurse with master’s
degree in nursing
2 years Completion of bachelor’s degree in nursing
Portugal General nurse 4 years Completion of secondary high school education; completion of the national
examinations in geology, biology, mathematics, physics, and chemistry
San Marino Nurse No data No data
Slovakia Nurse 3 years Completion of high school/vocational school education; be at least 18 years
old; and be medically fit
Practical nurse No data No data
Slovenia Registered nurse 3 years Completion of 10 years of general education with diploma or similar
certification
Spain General care nurse 4 years Varies by region
Switzerland Registered nurse 3 years 12 years of schooling; 9 years plus 3 years of apprenticeship is also possible
United
Kingdom
Adult nurse 3 years Vary based on educational institution
Note. RN=registered nurse.
TABLE C33
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Midwives in
Western and Central Europe
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Andorra Midwife 2–4 years State diploma in secondary education or equivalent
Austria Midwife 2 years Completion of bachelor’s degree; professional aptitude and medical fitness
Czech Republic Midwife No data General education of 10 years as attested to by diploma/certificate or equiv
-
alency and experience as a nurse responsible for general care
France Midwife 5 years No data
Germany Midwife No data Completion of secondary education or equivalent, or, if completed a 10-year
schooling program, has a secondary school degree or equivalent and com
-
pletion of requisite vocational training; proofs of fitness for the profession;
certificate of health not older than 3 months
Hungary Midwife No data No data
Ireland Midwife No data Standard applicants must have a Leaving Certificate examination and a
minimum grade of H5 in two higher level papers, and O6/H7 in four ordi
-
nary or higher level papers in the following subjects: Irish or English, math-
ematics, a laboratory science subject, and three other subjects. Otherwise,
they must be judged by the higher education institutions to have attained
equivalent minimum education.
Liechtenstein Midwife 3 years Completed basic education in accordance with the provisions of regulations
in a recognized institution or an outside regulated program, or has acquired
at least 3 years of professional experience in the health field

www.journalofnursingregulation.com 107Volume 10
•
Special Issue
•
January 2020
TABLE C33 (continued)
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Luxembourg Midwife 1.5–3 years Completion of 10 years’ general education or equivalent or evidence of pos
-
session of nursing diploma
Malta Midwife 1.5–3 years Completion of 10 years’ general education with diploma or similar
certification
Monaco Midwife 2 years No data
Netherlands Midwife No data No data
Slovakia Midwife 3 years Completion of high school/vocational school education; be at least 18 years
old; and be medically fit
Slovenia Registered Midwife 1.5–3 years Completion of 10 years’ general education or equivalent or evidence of pos
-
session of nursing diploma
Spain Midwife 2 years Completion of 4-year nursing degree and requisite experience as a nurse
(generally 2 years)
United
Kingdom
Midwife 3 years (adult
nurses may com
-
plete in 18
months)
Not available
TABLE C34
Types of Nurses and Duration of Nursing program and Requirements for Entry—Specialty
Nurses in Western and Central Europe
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Andorra Specialist nurse 2 years Must hold a registered nurse license
Austria Surgical nurse 7 months Qualification in nursing care as a nurse
Pediatric nurse 1 year Qualification in nursing care as a nurse
Psychiatric nurse 1 year Qualification in nursing care as a nurse
Czech Republic
(Czechia)
Child nurse No data General education of 10 years as attested to by diploma or certificate or
equivalency
France Psychiatric nurse No data No data
Nurse anesthetist 2 years Bachelor’s degree in nursing followed by state nurse certification for at least
2 years, followed by competition into specialized school for training
Operating room
nurse
1.5 years Bachelor’s degree in nursing followed by state nurse certification for at least
2 years, followed by competition into specialized school for training
Nursery nurse 1 year Bachelor’s degree in nursing followed by state nurse certification, followed
by competition into specialized school for training
Germany Nurse specialist 3 years Proofs of middle school diploma or another equivalently recognized degree;
secondary school diploma or equivalent or another completed 10-year
schooling training that complements the secondary school diploma;
successfully completed vocational training of at least 2 years; regulated as
-
sistance or helper training in care of at least 1 year; or permission as a medi-
cal nursing assistant or nursing assistant; or Hauptschulabschluss or one
equivalent recognized educational qualification; or,completed at least 1 year
of training in geriatric nursing assistant; or licensed as a nursing assistant.
There is a minimum age requirement; some schools set maximum age re
-
quirements, though a maximum age is not required by law.
Pediatric nurse 3 years Prequalification for a secondary education or for a secondary school diplo
-
ma or equivalent that the student has completed at least 2 years of voca-
tional training; has a nursing assistant license; or has successfully complet-
ed nationally regulated training of at least 1 year in the nursing assistant or
geriatric nursing assistant field. A vocational education is not legally re
-
quired for applicants with a medium level of education for students with a
high school diploma.
There is a minimum age requirement; some schools set maximum age re
-
quirements, though a maximum age is not required by law.

108 Journal of Nursing Regulation
TABLE C34 (continued)
Country Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Germany
(continued)
Geriatric nurse 3 years Proofs of middle school diploma or another equivalently recognized degree;
secondary school diploma or equivalent or another completed 10-year
schooling training that complements the Secondary school diploma;
successfully completed vocational training of at least 2 years; regulated as
-
sistance or helper training in care of at least 1 year; or permission as a medi-
cal nursing assistant or nursing assistant; or Hauptschulabschluss or one
equivalent recognized educational qualification; or completed at least 1 year
of training in geriatric nursing assistant; or licensed as a nursing assistant.
There is a minimum age requirement; some schools set maximum age re
-
quirements, though a maximum age is not required by law.
Hungary Occupational health
nurse
1 year Completion of secondary school; general nurse qualification; medical
certificate
Psychiatric nurse No data No data
Nurse practitioner No data No data
Luxembourg Psychiatric nurse 2 years State nursing diploma or recognition of nursing diploma obtained abroad
Pediatric nurse 2 years State nursing diploma or recognition of nursing diploma obtained abroad
Anesthesia and re
-
suscitation nurse
2 years State nursing diploma or recognition of nursing diploma obtained abroad
Medical technical
assistant
2 years State nursing diploma or recognition of nursing diploma obtained abroad
Malta Children’s nurse 1 or 3 years, de
-
pending on pro-
gram track
Completion of 10 years of general education with diploma or similar certifi
-
cation prior to 3-year children’s nursing program; or nursing diploma prior
to entry into special 12-month children’s nurse training
Mental health nurse 1 or 3 years, de
-
pending on pro-
gram track
Completion of 10 years of general education with diploma or similar certifi
-
cation prior to 3-year mental health nursing program; or nursing diploma
prior to entry into special 12-month mental health nurse training
Monaco Nurse anesthetist No data Nursing diploma
Portugal Specialist nurse in
community nursing
1–1.5 years Must hold degree of licentiate in nursing or equivalent as well as profes
-
sional title of nurse; and have at least 2 years of professional practice as a
nurse
Specialist nurse in
surgical nursing
1–1.5 years Must hold degree of licentiate in nursing or equivalent as well as profes
-
sional title of nurse; and have at least 2 years of professional practice as a
nurse
Specialist nurse in
Infant health and
pediatrics
1–1.5 years Must hold degree of licentiate in nursing or equivalent as well as profes
-
sional title of nurse; and have at least 2 years of professional practice as a
nurse
Portugal
(continued)
Specialist nurse in
maternal health and
obstetrics
1.5 years Must hold degree of licentiate in nursing or equivalent as well as profes-
sional title of nurse; and have at least 2 years of professional practice as a
nurse
Slovakia Advanced practice
nurse
2–3 years Completion of 4-year nursing degree or the equivalent and requisite experi
-
ence as a nurse (generally 2 years)
Spain Mental health nurse 2–3 years Completion of 4-year nursing degree or the equivalent and requisite experi
-
ence as a nurse (generally 2 years)
Spain Obstetric nurse 2–3 years Completion of 4-year nursing degree or the equivalent and requisite experi
-
ence as a nurse (generally 2 years)
Community nurse 2–3 years Completion of 4-year nursing degree or the equivalent and requisite experi
-
ence as a nurse (generally 2 years)
Pediatric nurse 2–3 years Completion of 4-year nursing degree or the equivalent and requisite experi
-
ence as a nurse (generally 2 years)
Specialist nurse 2–3 years Completion of 4-year nursing degree or the equivalent and requisite experi
-
ence as a nurse (generally 2 years)
Switzerland Nurse specialist 1–2 years Registered nursing diploma, plus work experience in different specialties
Advanced practice
nurse
2 years Bachelor of science in nursing degree; clinical competence and experience
United
Kingdom
Children’s nurse 1 year Completion of adult nurse program
Intellectual disability
nurse
1 year Completion of adult nurse program
Specialist nurse in
community nursing
1 year Completion of adult nurse program
Mental health nurse 1 year Completion of adult nurse program

www.journalofnursingregulation.com 109Volume 10
•
Special Issue
•
January 2020
Middle East
TABLE C35
Types of Nurses and Duration of Nursing Program and Requirements for Entry by Nurse—
Middle East
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Armenia Nurse (RN) 3 years Completion of high school education
Bahrain General nurse 3–4 years Completion of high school education
Georgia Practice nurse (Type 1) 3 years Secondary education
Practice nurse (Type 2) 4 years The National Entrance Examination
Iran General nurse 4 years No data
Iraq Nurse No data Completion of Grade 10
Israel RN 4 years in aca
-
demic program;
2.5 years for
diploma
High school diploma, citizen of Israel, psychometric examinations
Jordan RN 4 years Secondary certificate
Kuwait Nurse No data No data
Lebanon RN 3 years Completion of high school education (13 years of school)
Nurse 3 years Completion of Grade 9 (10 years of school)
Oman Nurse 3 years Students’ admission to nursing institutes and university nursing programs
is based on secondary school grades and demonstrating a proficiency of
the English language and admissions interviews in Arabic and English.
Palestine Nurse No data Completion of high school education
Saudi Arabia Nurse Bachelor’s pro
-
gram in nursing
Certificate of completion from the training of the concession year;
Copy of identification (national identity / passport / residence);
Recent personal photograph;
Academic record;
Must be medically fit;
Successful passage of the comprehensive acceptance test held by the
Commission;
Certificate of professional classification (if any) with mandatory classifica
-
tion after admission and before the start of the program;
Letter of preliminary approval to join the program from the approved em
-
ployer, and, in case of acceptance, to bring the final letter of completion for
the entire period of the program (for employees); and
Payment of fees (300 riyal) in the case of a request for re-evaluation of cur
-
riculum vitae
Syrian Arab
Republic
Nurse No data Requirements are determined by the Syrian Higher Education Council
United Arab
Emirates
RN 3 years No data
Note. RN=registered nurse.
TABLE C36
Types of Nurses and Duration of Nursing Program and Requirements for Entry—Specialist
Nurses in the Middle East
Jurisdiction Nurse Type Duration of Nursing
Program
Requirements for Entry Into Program
Armenia Nurse manager 4 years Completion of high school education
Bahrain Clinical nurse
specialist
Minimum of 500 hours
of clinical experience
Bachelor’s degree in nursing
Specialist nurse 1 year Qualification as a general nurse
Iran Nurse anesthetist 2 years No data
Operating room nurse 2 years No data

110 Journal of Nursing Regulation
TABLE C36 (continued)
Jurisdiction Nurse Type Duration of Nursing
Program
Requirements for Entry Into Program
Israel Clinical nurse
specialist
1 year RN; diploma, post-basic education, clinical experience
Academic registered
lactation consultant
Additional program,
following nursing di
-
ploma/degree
Is an RN
Post-basic nurse 1 year RN; diploma; bachelor of arts; entry examination
Lebanon Technique superior RN Prior to 2014: 3 years;
after 2014: 2 years,
plus 1 year of specialty
Completion of high school education or technical baccalaureate
Oman Psychiatric nurse No data Nursing degree, demonstrating a proficiency of the English lan
-
guage, and admissions interviews in Arabic and English
Infectious disease
nurse
No data Nursing degree, demonstrating a proficiency of the English lan
-
guage, and admissions interviews in Arabic and English
Pediatric nurse No data Nursing degree, demonstrating a proficiency of the English lan
-
guage and admissions interviews in Arabic and English
Saudi Arabia Nurse Specialist 1 1 year of excellence
program
Completion of bachelor’s program in specialty
Nurse Specialist 2 Additional required
expertise program
Master’s degree or equivalent in specialty
First Nurse Specialist 1 1 year of excellence
program
2 years of post-master’s degree nursing experience
Saudi Arabia
(continued)
First Nurse Specialist 2 Additional required
expertise program
3 years of post-master’s degree nursing experience
Advisory nurse/ PhD
nurse
Following a master’s
degree program in a
nursing specialty,
3 years of experience
in addition to PhD pro
-
gram (Doctor of Phi-
losophy) in nursing
Master’s degree or equivalent in a nursing specialty
United Arab
Emirates
Registered specialist
nurse
No data No data
Advanced practice
nurse
No data Completion of RN program
Note. RN=registered nurse.
TABLE C37
Types of Nurses and Duration of Nursing Programs and Requirements for Entry—Midwives
in the Middle East
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Azerbaijan Midwife (registered
midwife)
Up to 5 years Minimum high school education (Grade 10)
Nurse midwife Up to 5 years Minimum high school education (Grade 10)
Bahrain Midwife 9 months to 4
years (duration is
dependent on
program)
If seeking a postgraduate midwifery certificate, initial qualification as a gen
-
eral nurse is necessary
Iraq Midwife 3 years Completion of Grade 10
Jordan Midwife 4 years Secondary certificate
Kuwait Midwife No data No data
Oman Midwife No data Requires a nursing degree, demonstrating a proficiency of the English lan
-
guage, and admissions interviews in Arabic and English
Palestine Midwife No data Completion of high school education
Syrian Arab
Republic
Midwife No data Such requirements are determined by the Syrian Higher Education Council

www.journalofnursingregulation.com 111Volume 10
•
Special Issue
•
January 2020
TABLE C37 (continued)
Jurisdiction Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
United Arab
Emirates
Registered midwife No data No data
Yemen Midwife 3 years Minimum high school education (Grade 10)
Nurse midwife 3 years Minimum high school education (Grade 10)
TABLE C38
Types of Nurses and Duration of Nursing Programs and Requirements for Entry—Nurse
Assistants in the Middle East
Middle Eastern
Jurisdiction
Nurse Type Duration of Nurs-
ing Program
Requirements for Entry Into Program
Armenia Nurse assistant 1 year Completion of high school education
Azerbaijan Auxiliary midwife No data No data
Bahrain Practical nurse 1.5 years Completion of high school education
Georgia Nursing assistant 1.5–2 years Basic education, secondary education
Iran Practical nurse 12 years of gen
-
eral education
No data
Israel Practical nurse 1 year High school diploma, citizen of Israel, internal examinations
Jordan Practical nurse 2 years (Currently discontinued for new applicants)
Associated nurse 2 years Secondary certificate
Saudi Arabia Nursing assistant No data No data
United Arab
Emirates
Practical nurse No data No data
Practical midwife No data No data
Yemen Medical assistant No data No data

112 Journal of Nursing Regulation
APPENDIX D
Global Regulatory Atlas Questionnaire
Start of Block: Introduction
Thank you for contributing to the Global Regulatory Atlas project. Please answer the questions below as best you are able. If you have dif-
ficulty with this survey, please contact us at [email protected] for assistance.
We’d like to begin by asking about the regulation of nurses in your jurisdiction.
Please indicate if your country/province/state has the following ar-
rangements in place to facilitate mobility of nurses (allow nurses to
work across state, province, or country borders):
☐ Mutual agreements (with which other countries/provinces/
states?) ________________________________________________
☐ Regional compacts (please name) ________________________
______________________________________________________
☐ Neither of these
Is there a law or regulations related to the regulation or governance
of nursing in your country/state/province?
○ Yes
○ No
Where can they be found? Please provide a link if possible.
Is there a body that governs and regulates nursing in your country/
state/jurisdiction? We will refer to this body as the regulatory body.
○ Yes
○ No
What is the mandate of the body that has authority over nursing?
☐ Public protection
☐ Promotion of the nursing profession
☐ Workforce, labor, or union issues
☐ Other (please describe) __________________________________
______________________________________________________
We’d like to focus on the body that governs and regulates nursing,
which we’ll refer to as the “regulatory body.” Which best describes
this body?
○ The regulatory body for nursing is independent from the
bodies that regulate other professions.
○ The regulatory body for nursing is part of a multidisci
-
plinary body that regulates many professions.
○ Other (please describe) _______________________________
_____________________________________________________
Please give us the name of this organization and the name of its
leader:
Physical or postal address of the regulatory body:
Website of the regulatory body, if available:
End of Block: Introduction
Start of Block: Regulatory Body Composition
Please tell us about the composition of this regulatory body.
How many representatives serve on the regulatory body? Who is involved in serving as a representative on the regulatory
body?
☐ Nurses
☐ Physicians
☐ Public Members
☐ Others (please describe) _________________________________
_______________
www.journalofnursingregulation.com 113Volume 10
•
Special Issue
•
January 2020
How are representatives appointed to serve on the regulatory
body?
○ Elected
○ Nominated by profession and confirmed by government
○ Appointment process
○ Other (please describe) _______________________________
_________________
Are there any competencies or qualifications needed in order to
serve on the regulatory body?
What are the governance powers of this body?
☐ Licensing/registering nurses
☐ Administrating nursing law and regulations
☐ Making decisions about scope of practice
☐ Creating legislation
☐ Disciplining nurses
☐ Other (please describe) __________________________________
______________
End of Block: Regulatory Body Composition
Start of Block: Regulatory Body Operations
Next, we will ask about the operations of the regulatory body with authority over nurses.
Is there a publicly available database or register of all nurses?
○ Yes
○ No
Where can this database be found? Please provide a link if
possible.
How does the regulatory body store disciplinary records and data?
○ In the same database that contains nurse registry
information
○ In another database (please describe) __________________
______________________________
○ Other (please describe) _______________________________
_________________
○ We do not store disciplinary records
For how long are these records stored?
Are these records available to the public?
○ Yes
○ No
What is the range of available discipline options or actions that can
be taken against a nurse for conduct or competence reasons?
☐ Censure
☐ Cease and desist order
☐ Reprimand
☐ Summary suspension
☐ Suspension
☐ Remediation
☐ Citation Order
☐ Revocation
☐ Warnings
☐ Fine/civil penalty
☐ Practice limitation with probation
☐ Practice limitation without probation
☐ Probation
☐ Conditional probation
☐ Assessment of costs
☐ Community service
☐ Surrender of license
☐ Denial of license
☐ Other options not listed here (please specify) _____________
___________________________________
Does this regulatory body have the authority to require and desig
-
nate a required national/jurisdictional examination?
○ Yes
○ No
End of Block: Regulatory Body Operations

114 Journal of Nursing Regulation
Start of Block: Nursing Education
We would like to ask about nursing education in your jurisdiction.
Does the regulatory body have the authority to approve nursing
education schools or programs?
○ Yes
○ No
Who approves education programs, if not the regulatory body?
Are nursing programs accredited in your country/province/state?
○ Yes
○ No
Is accreditation of programs required?
○ Yes
○ No
End of Block: Nursing Education
Start of Block: Telehealth
Does your regulatory body have regulations or policies regarding
telehealth for nurses?
○ Yes
○ No
Are telehealth nursing services being provided to patients inside
this jurisdiction from outside this jurisdiction?
○ Yes
○ No
○ Unsure
Do nurses in this jurisdiction provide telehealth nursing services
across any international borders?
○ Yes
○ No
○ Unsure
End of Block: Telehealth
Start of Block: Nurse Type
We are now going to ask you about the nursing workforce in your country/state/province. In the lines below, please provide some informa-
tion about the different types of nurse in your country/state/province. If you have more types of nurses in your jurisdiction than the space
provides for, please contact us at [email protected] for assistance.
Type of
nurse
Credentials
used (RN,
RGN, etc.)
Number of
nurses of
this type
General re-
quirements
for entry into
educational
or training
program
Length of
educational
or training
program
National/ju
-
risdictional
examination
required, if
any
What medi
-
cations may
this type of
nurse pre
-
scribe, if
any?
May this
type of nurse
refer pa
-
tients to oth-
er services?
May this
type of nurse
diagnose?

www.journalofnursingregulation.com 115Volume 10
•
Special Issue
•
January 2020
How is recognition or authority to practice granted in your country/
state/province?
○ Licensure
○ Registration
○ Considered authorized when education is completed
○ Another way (please describe) _________________________
_______________________
Does your country/state/province require nurses from other coun
-
tries to pass a language proficiency examination?
○ Yes
○ No
What language proficiency examinations are accepted?
Is evidence of good moral character required?
○ Yes
○ No
Please describe the evidence of good moral character that is
required.
If a nurse from another country wishes to practice as a nurse in
your country/state/province, describe the process they would fol
-
low to become authorized.
Are there requirements for proof of continuing competence or con
-
tinuing fitness to practice?
○ Yes
○ No
What are the requirements for proof of continuing competence or
fitness to practice?
How often must these requirements be completed?
Are there any additional requirements for nurses that we have not
previously mentioned?
End of Block: Nurse Type
Start of Block: Block 6
Finally, we have a few questions about nursing research in your jurisdiction.
Does the regulatory body undertake regulatory research?
○ Yes
○ No
What are the major research priorities?
End of Block: Block 6

116 Journal of Nursing Regulation
